

Methicillin-resistant Staphylococcus aureus transmission and infections in a neonatal intensive care unit despite active surveillance cultures and decolonization: challenges for infection prevention
- PMID: 24602947
- PMCID: PMC3950943
- DOI: 10.1086/675594
Methicillin-resistant Staphylococcus aureus transmission and infections in a neonatal intensive care unit despite active surveillance cultures and decolonization: challenges for infection prevention
Abstract
Objective: To characterize the epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) transmission and infections in a level IIIC neonatal intensive care unit (NICU) and identify barriers to MRSA control.
Setting and design: Retrospective cohort study in a university-affiliated NICU with an MRSA control program including weekly nares cultures of all neonates and admission nares cultures for neonates transferred from other hospitals or admitted from home.
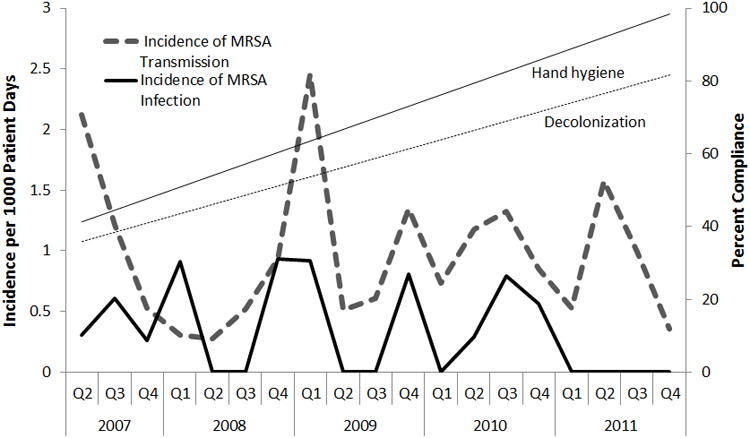
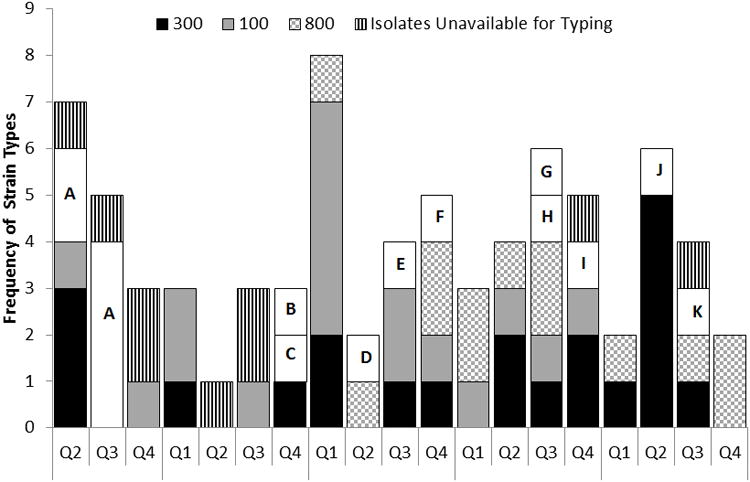
Methods: Medical records were reviewed to identify neonates with NICU-acquired MRSA colonization or infection between April 2007 and December 2011. Compliance with hand hygiene and an MRSA decolonization protocol were monitored. Relatedness of MRSA strains were assessed using pulsed-field gel electrophoresis (PFGE).
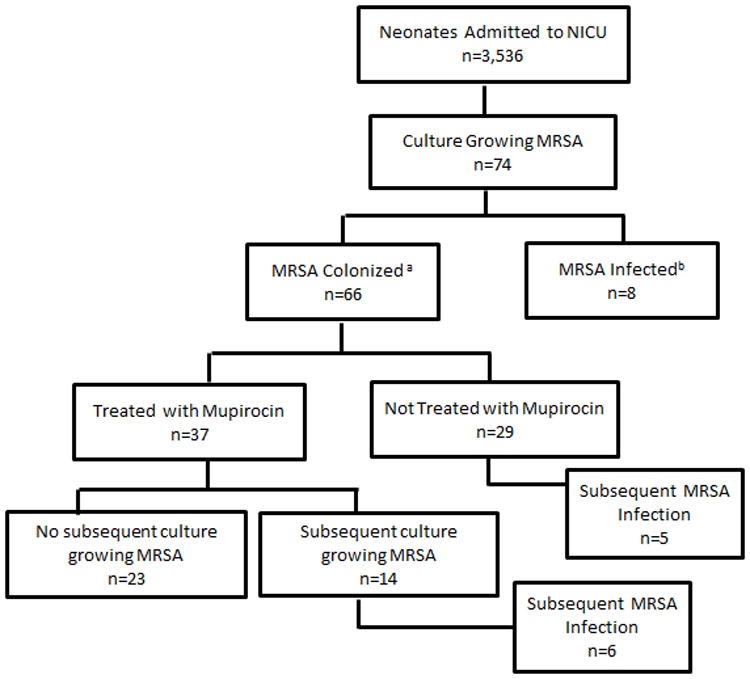
Results: Of 3,536 neonates, 74 (2.0%) had a culture grow MRSA, including 62 neonates with NICU-acquired MRSA. Nineteen of 74 neonates (26%) had an MRSA infection, including 8 who became infected before they were identified as MRSA colonized, and 11 of 66 colonized neonates (17%) developed a subsequent infection. Of the 37 neonates that underwent decolonization, 6 (16%) developed a subsequent infection, and 7 of 14 (50%) that remained in the NICU for 21 days or more became recolonized with MRSA. Using PFGE, there were 14 different strain types identified, with USA300 being the most common (31%).
Conclusions: Current strategies to prevent infections-including active identification and decolonization of MRSA-colonized neonates-are inadequate because infants develop infections before being identified as colonized or after attempted decolonization. Future prevention efforts would benefit from improving detection of MRSA colonization, optimizing decolonization regimens, and identifying and interrupting reservoirs of transmission.
Conflict of interest statement
Potential conflicts of interest: All other authors report no disclosures.
Figures
References
-
- Stoll BJ, Hansen NI, Adams-Chapman I, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA. 2004;292(19):2357–2365. - PubMed
-
- Schlapbach LJ, Aebischer M, Adams M, et al. Impact of Sepsis on Neurodevelopmental Outcome in a Swiss National Cohort of Extremely Premature Infants. Pediatrics. 2011;128(2):e348–e357. - PubMed
-
- Hocevar SN, Edwards JR, Horan TC, Morrell GC, Iwamoto M, Lessa FC. Device-associated infections among neonatal intensive care unit patients: incidence and associated pathogens reported to the National Healthcare Safety Network, 2006-2008. Infect Control Hosp Epidemiol. 2012;33(12):1200–1206. - PMC - PubMed
-
- Lessa FC, Edwards JR, Fridkin SK, Tenover FC, Horan TC, Gorwitz RJ. Trends in incidence of late-onset methicillin-resistant Staphylococcus aureus infection in neonatal intensive care units: data from the National Nosocomial Infections Surveillance System, 1995-2004. Pediatr Infect Dis J. 2009;28(7):577–581. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous