

Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: pragmatic, factorial, randomised controlled trial
- PMID: 24603565
- PMCID: PMC3944682
- DOI: 10.1136/bmj.g1606
Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: pragmatic, factorial, randomised controlled trial
Abstract
Objective: To estimate the effectiveness of different strategies involving delayed antibiotic prescription for acute respiratory tract infections.
Design: Open, pragmatic, parallel group, factorial, randomised controlled trial.
Setting: Primary care in the United Kingdom.
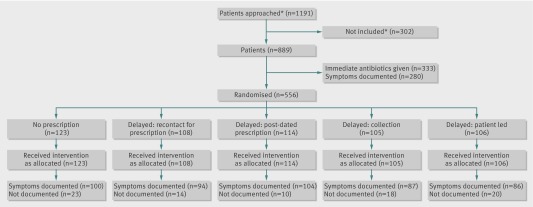
Patients: 889 patients aged 3 years and over with acute respiratory tract infection, recruited between 3 March 2010 and 28 March 2012 by 53 health professionals in 25 practices.
Interventions: Patients judged not to need immediate antibiotics were randomised to undergo four strategies of delayed prescription: recontact for a prescription, post-dated prescription, collection of the prescription, and be given the prescription (patient led). During the trial, a strategy of no antibiotic prescription was added as another randomised comparison. Analysis was intention to treat.
Main outcome measures: Mean symptom severity (0-6 scale) at days 2-4 (primary outcome), antibiotic use, and patients' beliefs in the effectiveness of antibiotic use. Secondary analysis included comparison with immediate use of antibiotics.
Results: Mean symptom severity had minimal differences between the strategies involving no prescription and delayed prescription (recontact, post-date, collection, patient led; 1.62, 1.60, 1.82, 1.68, 1.75, respectively; likelihood ratio test χ(2) 2.61, P=0.625). Duration of symptoms rated moderately bad or worse also did not differ between no prescription and delayed prescription strategies combined (median 3 days v 4 days; 4.29, P=0.368). There were modest and non-significant differences in patients very satisfied with the consultation between the randomised groups (79%, 74%, 80%, 88%, 89%, respectively; likelihood ratio test χ(2) 2.38, P=0.667), belief in antibiotics (71%, 74%, 73%, 72%, 66%; 1.62, P=0.805), or antibiotic use (26%, 37%, 37%, 33%, 39%; 4.96, P=0.292). By contrast, most patients given immediate antibiotics used antibiotics (97%) and strongly believed in them (93%), but with no benefit for symptom severity (score 1.76) or duration (median 4 days).
Conclusion: Strategies of no prescription or delayed antibiotic prescription result in fewer than 40% of patients using antibiotics, and are associated with less strong beliefs in antibiotics, and similar symptomatic outcomes to immediate prescription. If clear advice is given to patients, there is probably little to choose between the different strategies of delayed prescription.
Trial registration: ISRCTN38551726.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
[Delayed antibiotic prescription for respiratory tract infections? - Delayed antibiotic prescription and no prescription lead to similar outcomes].Dtsch Med Wochenschr. 2014 May;139(17):874. doi: 10.1055/s-0033-1353900. Epub 2014 Apr 23. Dtsch Med Wochenschr. 2014. PMID: 24760687 German. No abstract available.
-
Delayed prescribing for respiratory tract infections in primary care results in lower antibiotic use.Evid Based Med. 2014 Oct;19(5):197. doi: 10.1136/eb-2014-110012. Epub 2014 Jun 5. Evid Based Med. 2014. PMID: 24904024 No abstract available.
References
-
- Goossens H, Ferech M, Vander Stichele R, Elseviers M, ESAC project group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 2005;365:579-87. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay A. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010;340:c2096. - PubMed
-
- House of Lords. House of Lords Select Committee on Science and Technology: 7th report. Occasional Report 1998.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials