

Perinatal outcomes for extremely preterm babies in relation to place of birth in England: the EPICure 2 study
- PMID: 24604108
- PMCID: PMC3995269
- DOI: 10.1136/archdischild-2013-305555
Perinatal outcomes for extremely preterm babies in relation to place of birth in England: the EPICure 2 study
Abstract
Background: Expertise and resources may be important determinants of outcome for extremely preterm babies. We evaluated the effect of place of birth and perinatal transfer on survival and neonatal morbidity within a prospective cohort of births between 22 and 26 weeks of gestation in England during 2006.
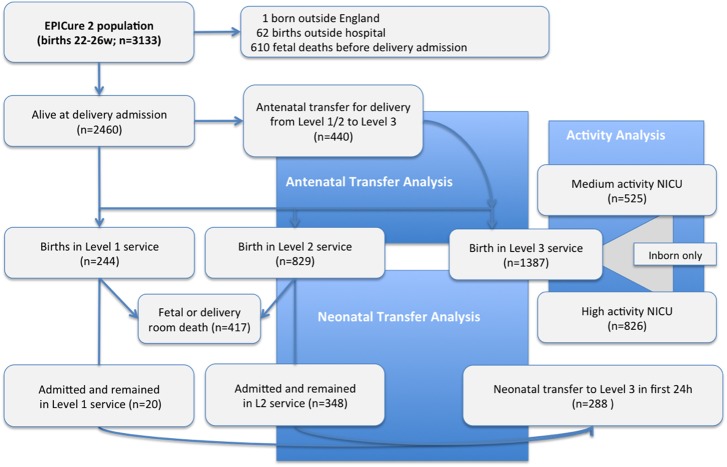
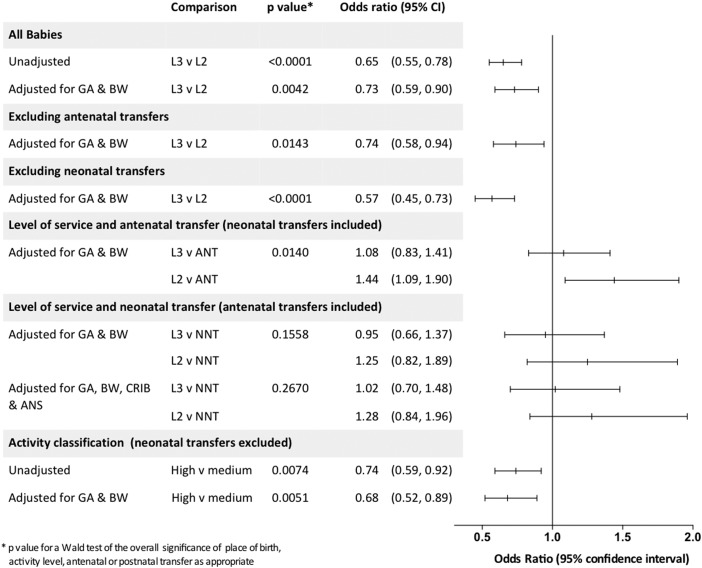
Methods: We studied the whole population of 2460 births where the fetus was alive at the admission of the mother to hospital for delivery. Outcomes to discharge were compared between level 3 (most intensive) and level 2 maternity services, with and without transfers, and by activity level of level 3 neonatal unit; ORs were adjusted for gestation at birth and birthweight for gestation (adjusted ORs (aOR)).
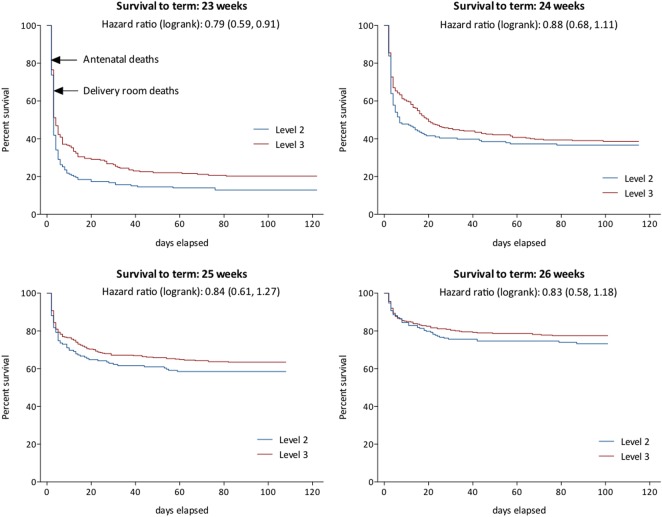
Findings: Of this national birth cohort, 56% were born in maternity services with level 3 and 34% with level 2 neonatal units; 10% were born in a setting without ongoing intensive care facilities (level 1). When compared with level 2 settings, risk of death in level 3 services was reduced (aOR 0.73 (95% CI 0.59 to 0.90)), but the proportion surviving without neonatal morbidity was similar (aOR 1.27 (0.93 to 1.74)). Analysis by intended hospital of birth confirmed reduced mortality in level 3 services. Following antenatal transfer into a level 3 setting, there were fewer intrapartum or labour ward deaths, and overall mortality was higher for those remaining in level 2 services (aOR 1.44 (1.09 to 1.90)). Among level 3 services, those with higher activity had fewer deaths overall (aOR 0.68 (0.52 to 0.89)).
Interpretation: Despite national policy, only 56% of births between 22 and 26 weeks of gestation occurred in maternity services with a level 3 neonatal facility. Survival was significantly enhanced following birth in level 3 services, particularly those with high activity; this was not at the cost of increased neonatal morbidity.
Keywords: Epidemiology; Neonatology.
Figures
Comment in
-
Perinatal outcomes.Arch Dis Child Fetal Neonatal Ed. 2014 Nov;99(6):F521. doi: 10.1136/archdischild-2014-307338. Epub 2014 Sep 23. Arch Dis Child Fetal Neonatal Ed. 2014. PMID: 25249189 No abstract available.
References
-
- Lasswell SM, Barfield WD, Rochat RW, et al. Perinatal regionalization for very low-birth-weight and very preterm infants: a meta-analysis. JAMA 2010;304: 992–1000 - PubMed
-
- Department of Health. Report of DH Expert Working Group on neonatal intensive care services. London: Department of Health, 2003
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources