

Management of borderline and locally advanced pancreatic cancer: where do we stand?
- PMID: 24605025
- PMCID: PMC3942831
- DOI: 10.3748/wjg.v20.i9.2255
Management of borderline and locally advanced pancreatic cancer: where do we stand?
Abstract
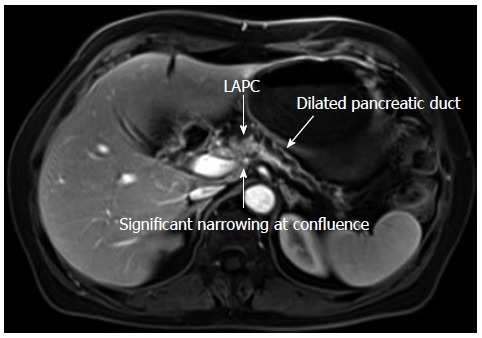
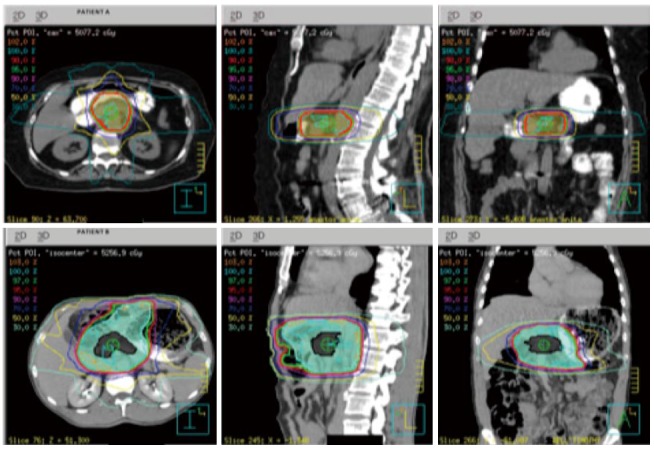
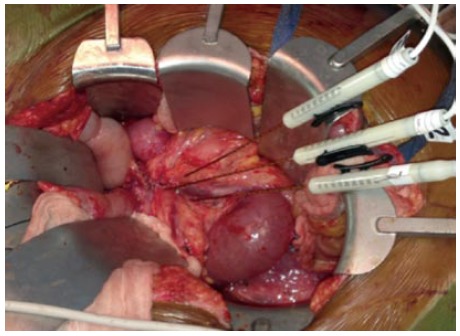
Many patients with pancreas cancer present with locally advanced pancreatic cancer (LAPC). The principle tools used for diagnosis and staging of LAPC include endoscopic ultrasound, axial imaging with computed tomography and magnetic resonance imaging, and diagnostic laparoscopy. The definition of resectability has historically been vague, as there is considerable debate and controversy as to the definition of LAPC. For the patient with LAPC, there is some level of involvement of the surrounding vascular structures, which include the superior mesenteric artery, celiac axis, hepatic artery, superior mesenteric vein, or portal vein. When feasible, most surgeons would recommend possible surgical resection for patients with borderline LAPC, with the goal of an R0 resection. For initially unresectable LAPC, neoadjuvant should be strongly considered. Specifically, these patients should be offered neoadjuvant therapy, and the tumor should be assessed for possible response and eventual resection. The efficacy of neoadjuvant therapy with this approach as a bridge to potential curative resection is broad, ranging from 3%-79%. The different modalities of neoadjuvant therapy include single or multi-agent chemotherapy combined with radiation, chemotherapy alone, and chemotherapy followed by chemotherapy with radiation. This review focuses on patients with LAPC and addresses recent advances and controversies in the field.
Keywords: Chemotherapy; Irreversible electroporation; Locally advanced; Pancreas; Pancreatic cancer; Radiation.
Figures


References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Tuveson DA, Neoptolemos JP. Understanding metastasis in pancreatic cancer: a call for new clinical approaches. Cell. 2012;148:21–23. - PubMed
-
- Kircher SM, Krantz SB, Nimeiri HS, Mulcahy MF, Munshi HG, Benson AB. Therapy of locally advanced pancreatic adenocarcinoma: unresectable and borderline patients. Expert Rev Anticancer Ther. 2011;11:1555–1565. - PubMed
-
- Calvo F, Guillen Ponce C, Muñoz Beltran M, Sanjuanbenito Dehesa A. Multidisciplinary management of locally advanced-borderline resectable adenocarcinoma of the head of the pancreas. Clin Transl Oncol. 2013;15:173–181. - PubMed
-
- Evans DB, Farnell MB, Lillemoe KD, Vollmer C, Strasberg SM, Schulick RD. Surgical treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol. 2009;16:1736–1744. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
