

Minimally invasive radical pancreatectomy for left-sided pancreatic cancer: current status and future perspectives
- PMID: 24605031
- PMCID: PMC3942837
- DOI: 10.3748/wjg.v20.i9.2343
Minimally invasive radical pancreatectomy for left-sided pancreatic cancer: current status and future perspectives
Abstract
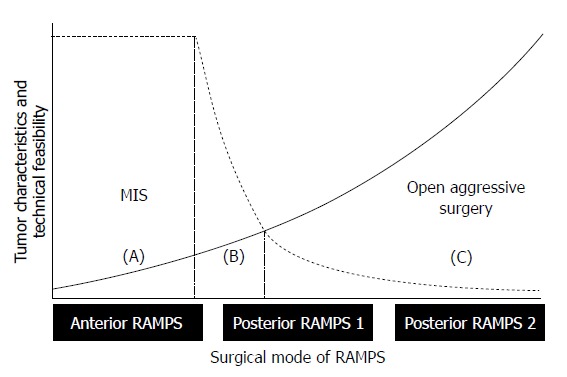
Minimally invasive distal pancreatectomy with splenectomy has been regarded as a safe and effective treatment for benign and borderline malignant pancreatic lesions. However, its application for left-sided pancreatic cancer is still being debated. The clinical evidence for radical antegrade modular pancreatosplenectomy (RAMPS)-based minimally invasive approaches for left-sided pancreatic cancer was reviewed. Potential indications and surgical concepts for minimally invasive RAMPS were suggested. Despite the limited clinical evidence for minimally invasive distal pancreatectomy in left-sided pancreatic cancer, the currently available clinical evidence supports the use of laparoscopic distal pancreatectomy under oncologic principles in well-selected left sided pancreatic cancers. A pancreas-confined tumor with an intact fascia layer between the pancreas and left adrenal gland/kidney positioned more than 1 or 2 cm away from the celiac axis is thought to constitute a good condition for the use of margin-negative minimally invasive RAMPS. The use of minimally invasive (laparoscopic or robotic) anterior RAMPS is feasible and safe for margin-negative resection in well-selected left-sided pancreatic cancer. The oncologic feasibility of the procedure remains to be determined; however, the currently available interim results indicate that even oncologic outcomes will not be inferior to those of open radical distal pancreatosplenectomy.
Keywords: Laparoscopic pancreatectomy, Robotic pancreatectomy; Pancreatic cancer.
Figures

References
-
- Nguyen NT, Hinojosa MW, Smith BR, Chang KJ, Gray J, Hoyt D. Minimally invasive esophagectomy: lessons learned from 104 operations. Ann Surg. 2008;248:1081–1091. - PubMed
-
- Shimizu S, Uchiyama A, Mizumoto K, Morisaki T, Nakamura K, Shimura H, Tanaka M. Laparoscopically assisted distal gastrectomy for early gastric cancer: is it superior to open surgery. Surg Endosc. 2000;14:27–31. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
