

Noninvasive prenatal diagnosis of congenital adrenal hyperplasia using cell-free fetal DNA in maternal plasma
- PMID: 24606108
- PMCID: PMC4037720
- DOI: 10.1210/jc.2014-1118
Noninvasive prenatal diagnosis of congenital adrenal hyperplasia using cell-free fetal DNA in maternal plasma
Abstract
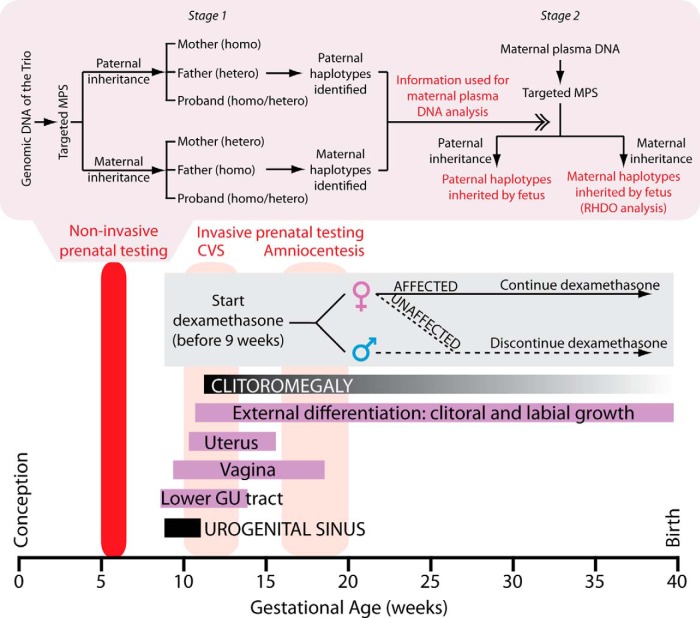
Context: Congenital adrenal hyperplasia (CAH) is an autosomal recessive condition that arises from mutations in CYP21A2 gene, which encodes for the steroidogenic enzyme 21-hydroxylase. To prevent genital ambiguity in affected female fetuses, prenatal treatment with dexamethasone must begin on or before gestational week 9. Currently used chorionic villus sampling and amniocentesis provide genetic results at approximately 14 weeks of gestation at the earliest. This means that mothers who want to undergo prenatal dexamethasone treatment will be unnecessarily treating seven of eight fetuses (males and three of four unaffected females), emphasizing the desirability of earlier genetic diagnosis in utero.
Objective: The objective of the study was to develop a noninvasive method for early prenatal diagnosis of fetuses at risk for CAH.
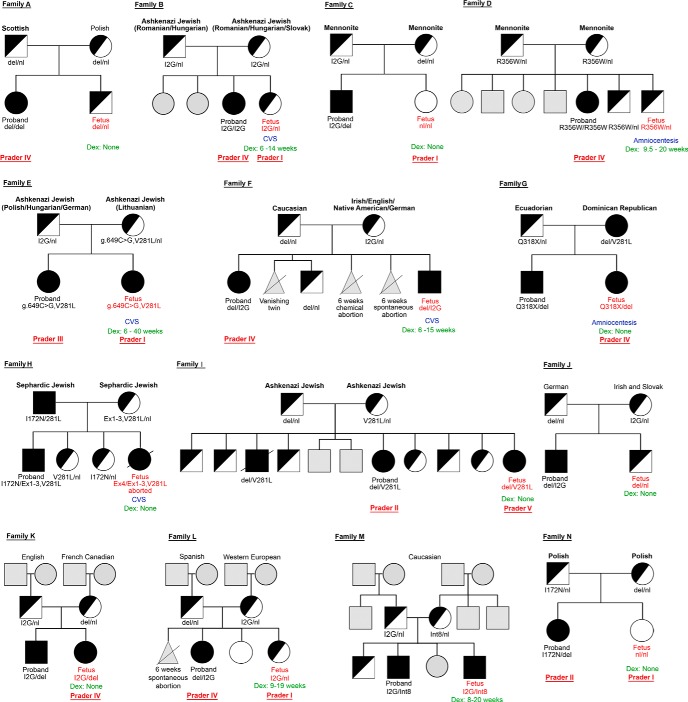
Patients: Fourteen families, each with a proband affected by phenotypically classical CAH, were recruited.
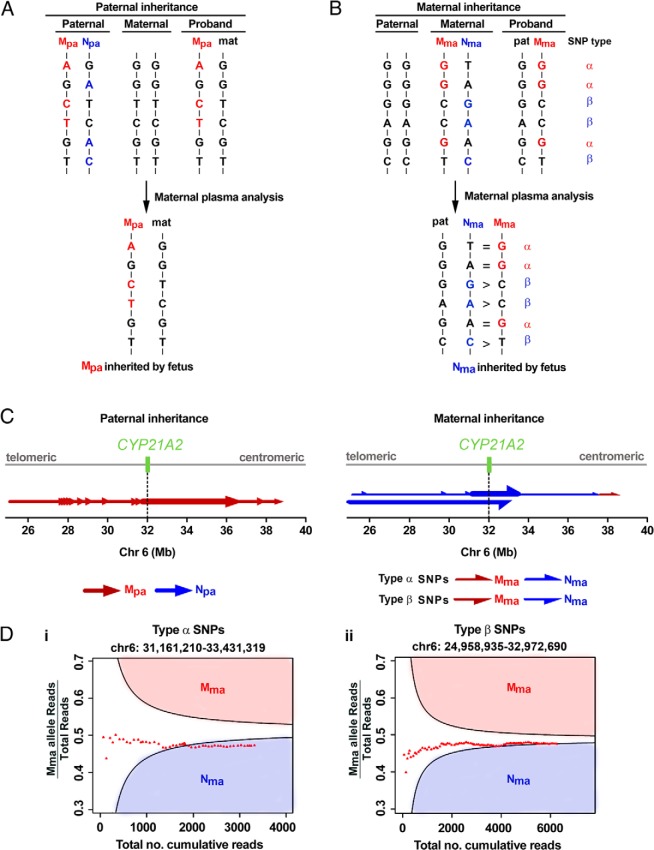
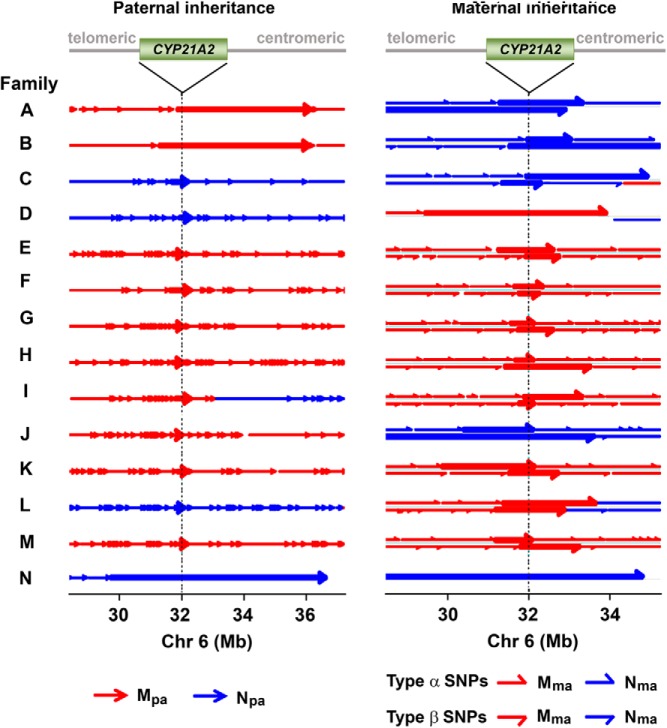
Design: Cell-free fetal DNA was obtained from 3.6 mL of maternal plasma. Using hybridization probes designed to capture a 6-Mb region flanking CYP21A2, targeted massively parallel sequencing (MPS) was performed to analyze genomic DNA samples from parents and proband to determine parental haplotypes. Plasma DNA from pregnant mothers also underwent targeted MPS to deduce fetal inheritance of parental haplotypes.
Results: In all 14 families, the fetal CAH status was correctly deduced by targeted MPS of DNA in maternal plasma, as early as 5 weeks 6 days of gestation.
Conclusions: MPS on 3.6 mL plasma from pregnant mothers could potentially provide the diagnosis of CAH, noninvasively, before the ninth week of gestation. Only affected female fetuses will thus be treated. Our strategy represents a generic approach for noninvasive prenatal testing for an array of autosomal recessive disorders.
Figures
References
-
- Pang SY, Wallace MA, Hofman L, et al. Worldwide experience in newborn screening for classical congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Pediatrics. 1988;81:866–874 - PubMed
-
- New MI, Lekarev O, Mancenido D, Parsa A, Yuen T. Congenital adrenal hyperplasia owing to 21-hydroxylase deficiency. In: New MI, Lekarev O, Parsa A, Yuen T, O'Malley BW, Hammer GD, eds. Genetic Steroid Disorders. London: Elsevier; 2014:29–51
-
- New MI, Abraham M, Yuen T, Lekarev O. An update on prenatal diagnosis and treatment of congenital adrenal hyperplasia. Semin Reprod Med. 2012;30:396–399 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
