

Trajectories of lung function during childhood
- PMID: 24606581
- PMCID: PMC4098108
- DOI: 10.1164/rccm.201309-1700OC
Trajectories of lung function during childhood
Abstract
Rationale: Developmental patterns of lung function during childhood may have major implications for our understanding of the pathogenesis of respiratory disease throughout life.
Objectives: To explore longitudinal trajectories of lung function during childhood and factors associated with lung function decline.
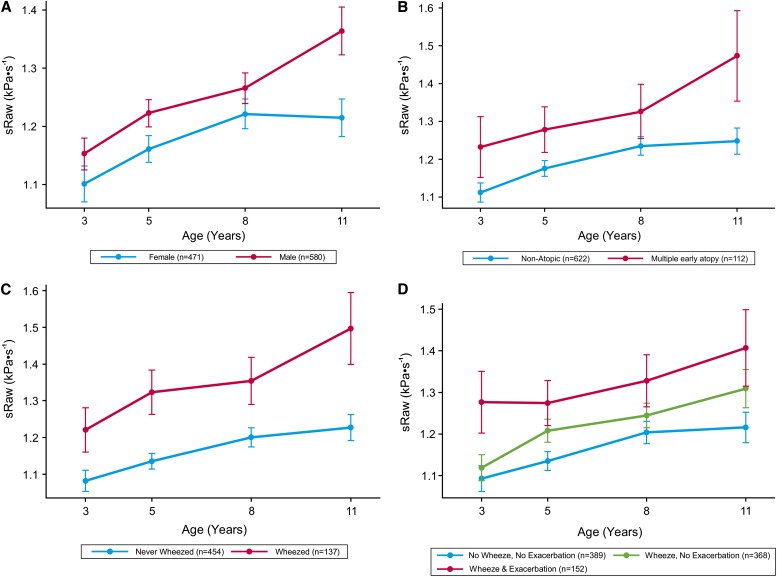
Methods: In a population-based birth cohort, specific airway resistance (sRaw) was assessed at age 3 (n = 560), 5 (n = 829), 8 (n = 786), and 11 years (n = 644). Based on prospective data (questionnaires, skin tests, IgE), children were assigned to wheeze phenotypes (no wheezing, transient, late-onset, and persistent) and atopy phenotypes (no atopy, dust mite, non-dust mite, multiple early, and multiple late). We used longitudinal linear mixed models to determine predictors of change in sRaw over time.
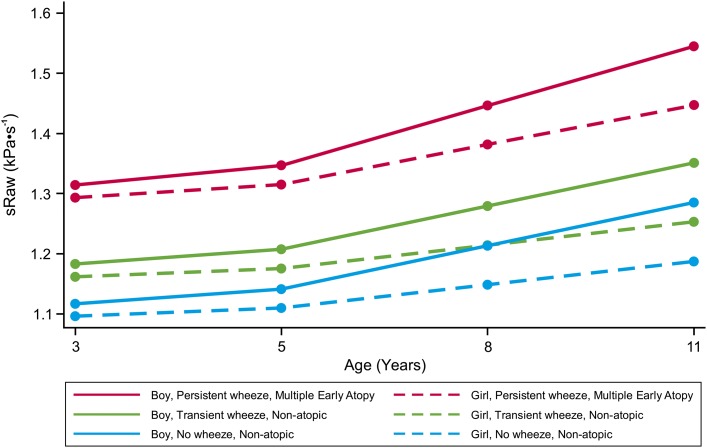
Measurements and main results: Contrary to the assumption that sRaw is independent of age and sex, boys had higher sRaw than girls (mean difference, 0.080; 95% confidence interval [CI], 0.049-0.111; P < 0.001) and a higher rate of increase over time. For girls, sRaw increased by 0.017 kPa ⋅ s(-1) per year (95% CI, 0.011-0.023). In boys this increase was significantly greater (P = 0.012; mean between-sex difference, 0.011 kPa ⋅ s(-1); 95% CI, 0.003-0.019). Children with persistent wheeze (but not other wheeze phenotypes) had a significantly greater rate of deterioration in sRaw over time compared with never wheezers (P = 0.009). Similarly, children with multiple early, but not other atopy phenotypes had significantly poorer lung function than those without atopy (mean difference, 0.116 kPa ⋅ s(-1); 95% CI, 0.065-0.168; P < 0.001). sRaw increased progressively with the increasing number of asthma exacerbations.
Conclusions: Children with persistent wheeze, frequent asthma exacerbations, and multiple early atopy have diminished lung function throughout childhood, and are at risk of a progressive loss of lung function from age 3 to 11 years. These effects are more marked in boys.
Figures
Comment in
-
Predictors of specific airway resistance during childhood.Am J Respir Crit Care Med. 2014 May 1;189(9):1019-21. doi: 10.1164/rccm.201403-0543ED. Am J Respir Crit Care Med. 2014. PMID: 24787064 Free PMC article. No abstract available.
References
-
- Sears MR, Greene JM, Willan AR, Wiecek EM, Taylor DR, Flannery EM, Cowan JO, Herbison GP, Silva PA, Poulton R. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414–1422. - PubMed
-
- Martinez FD, Morgan WJ, Wright AL, Holberg CJ, Taussig LM. Diminished lung function as a predisposing factor for wheezing respiratory illness in infants. N Engl J Med. 1988;319:1112–1117. - PubMed
-
- Turner SW, Palmer LJ, Rye PJ, Gibson NA, Judge PK, Young S, Landau LI, Le Souëf PN. Infants with flow limitation at 4 weeks: outcome at 6 and 11 years. Am J Respir Crit Care Med. 2002;165:1294–1298. - PubMed
-
- Doershuk CF, Fisher BJ, Matthews LW. Specific airway resistance from the perinatal period into adulthood. Alterations in childhood pulmonary disease. Am Rev Respir Dis. 1974;109:452–457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
