

Systematic review of percutaneous closure versus medical therapy in patients with cryptogenic stroke and patent foramen ovale
- PMID: 24607561
- PMCID: PMC3948581
- DOI: 10.1136/bmjopen-2013-004282
Systematic review of percutaneous closure versus medical therapy in patients with cryptogenic stroke and patent foramen ovale
Abstract
Objectives: To provide a comprehensive comparison of patent foramen ovale (PFO) closure versus medical therapy in patients with cryptogenic stroke or transient ischaemic attack (TIA) and demonstrated PFO.
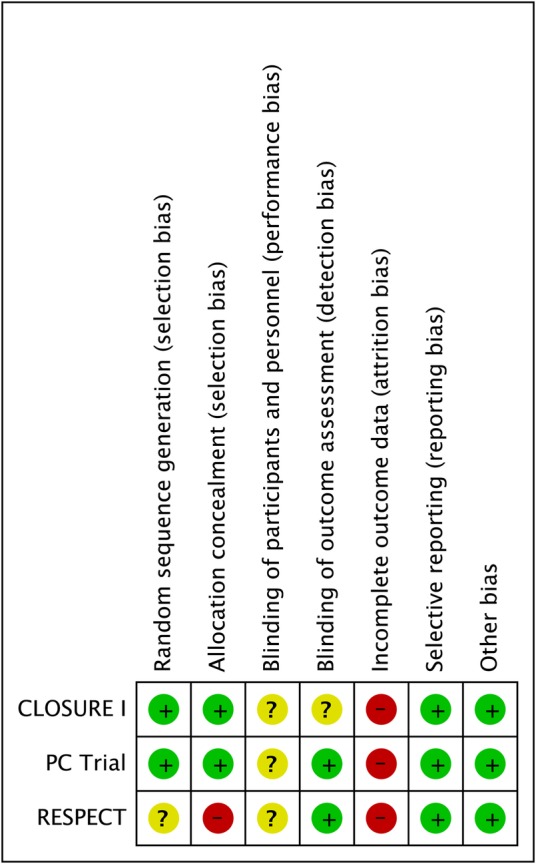
Design: Systematic review with complete case meta-analysis and sensitivity analyses. Data sources included MEDLINE and EMBASE from 1980 up to May 2013. All randomised controlled trials (RCTs) comparing treatment with percutaneous catheter-based closure of PFO to anticoagulant or antiplatelet therapy in patients with cryptogenic stroke or TIA and echocardiographically confirmed PFO or atrial septal defect (ASD) were eligible.
Participants: 1967 participants with prior stroke or TIA and echocardiographically confirmed PFO or ASD.
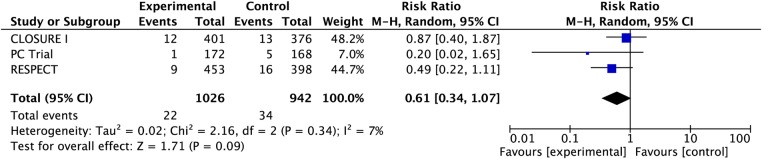
Primary outcome measures: The primary outcome of interest was recurrence of ischaemic stroke. We utilised data from complete cases only for the primary endpoint and combined data from trials to estimate the pooled risk ratio (RR) and associated 95% CIs calculated using random effects models.
Results: We identified 284 potentially eligible articles of which three RCTs including 2303 patients proved eligible and 1967 patients had complete data. Of the 1026 patients randomised to PFO closure and followed to study conclusion 22 experienced non-fatal ischaemic strokes, as did 34 of 941 patients randomised to medical therapy (risk ratio (RR) 0.61, 95% CI 0.34 to 1.07; heterogeneity: p=0.34, I(2)=8%, confidence in estimates low due to risk of bias and imprecision). Analyses for ischaemic stroke restricted to 'per-protocol' patients or patients with concomitant atrial septal aneurysm did not substantially change the observed RRs. Complication rates associated with either PFO closure or medical therapy were low.
Conclusions: Pooled data from three RCTs provides insufficient support that PFO closure is preferable to medical therapy for secondary prevention of cryptogenic stroke in patients with PFO.
Figures
References
-
- Webster MW, Chancellor AM, Smith HJ, et al. Patent foramen ovale in young stroke patients. Lancet 1988;2:11–12 - PubMed
-
- Lechat P, Mas JL, Lascault G, et al. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 1988;318:1148–52 - PubMed
-
- Khairy P, O'Donnell CP, Landzberg MJ. Transcatheter closure versus medical therapy of patent foramen ovale and presumed paradoxical thromboemboli: a systematic review. Ann Intern Med 2003;139:753–60 - PubMed
-
- Furlan AJ, Reisman M, Massaro J, et al. Closure or medical therapy for cryptogenic stroke with patent foramen ovale. N Engl J Med 2012;366:991–9 - PubMed
-
- Carroll JD, Saver JL, Thaler DE, et al. Closure of patent foramen ovale versus medical therapy after cryptogenic stroke. N Engl J Med 2013;368:1092–100 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical