

Human leukocyte antigen genes and interferon beta preparations influence risk of developing neutralizing anti-drug antibodies in multiple sclerosis
- PMID: 24608124
- PMCID: PMC3946519
- DOI: 10.1371/journal.pone.0090479
Human leukocyte antigen genes and interferon beta preparations influence risk of developing neutralizing anti-drug antibodies in multiple sclerosis
Abstract
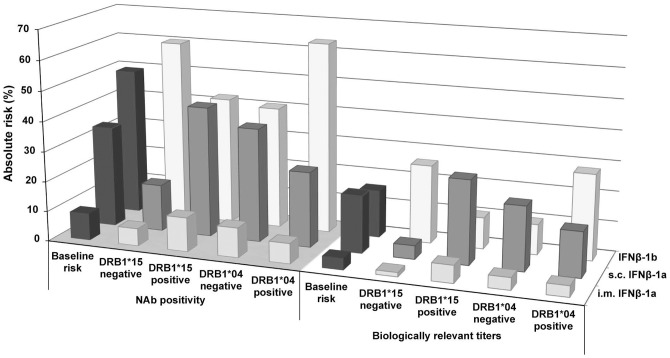
A significant proportion of patients with multiple sclerosis who receive interferon beta (IFNβ) therapy develop neutralizing antibodies (NAbs) that reduce drug efficacy. To investigate if HLA class I and II alleles are associated with development of NAbs against IFNβ we analyzed whether NAb status and development of NAb titers high enough to be biologically relevant (>150 tenfold reduction units/ml) correlated with the HLA allele group carriage in a cohort of 903 Swedish patients with multiple sclerosis treated with either intramuscular IFNβ-1a, subcutaneous IFNβ-1a or subcutaneous IFNβ-1b. Carriage of HLA-DRB1*15 was associated with increased risk of developing NAbs and high NAb titers. After stratification based on type of IFNβ preparation, HLA-DRB1*15 carriage was observed to increase the risk of developing NAbs as well as high NAb titers against both subcutaneous and intramuscular IFNβ-1a. Furthermore, in patients receiving subcutaneous IFNβ-1a carriage of HLA-DQA1*05 decreased the risk for high NAb titers. In IFNβ-1b treated patients, HLA-DRB1*04 increased the risk of developing high NAb titers, and in a subgroup analysis of DRB1*04 alleles the risk for NAbs was increased in DRB1*04:01 carriers. In conclusion, there is a preparation-specific genetically determined risk to develop NAbs against IFNβ high enough to be clinically relevant in treatment decisions for patients with multiple sclerosis if confirmed in future studies. However, choice of IFNβ preparation still remains the single most significant determinant for the risk of developing NAbs.
Conflict of interest statement
Figures
References
-
- PRISM Study Group, University of British Columbia MS/MRI Analysis Group (2001) PRISMS-4: Long-term efficacy of interferon-beta-1a in relapsing MS. Neurology 56: 1628–1636. - PubMed
-
- MS Study Group (1993) Interferon beta-1b is effective in relapsing-remitting multiple sclerosis. I. Clinical results of a multicenter, randomized, double-blind, placebo-controlled trial. The IFNB Multiple Sclerosis Study Group. Neurology 43: 655–661. - PubMed
-
- Jacobs LD, Cookfair DL, Rudick RA, Herndon RM, Richert JR, et al. (1996) Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Ann Neurol 39: 285–294. - PubMed
-
- Hesse D, Sellebjerg F, Sorensen PS (2009) Absence of MxA induction by interferon beta in patients with MS reflects complete loss of bioactivity. Neurology 73: 372–377. - PubMed
-
- Sominanda A, Hillert J, Fogdell-Hahn A (2008) In vivo bioactivity of interferon-beta in multiple sclerosis patients with neutralising antibodies is titre-dependent. J Neurol Neurosurg Psychiatry 79: 57–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
