

Early-stage rectal cancer: clinical and pathologic prognostic markers of time to local recurrence and overall survival after resection
- PMID: 24608301
- PMCID: PMC3954982
- DOI: 10.1097/DCR.0b013e3182a70709
Early-stage rectal cancer: clinical and pathologic prognostic markers of time to local recurrence and overall survival after resection
Abstract
Background: Resection without adjuvant therapy results in a low recurrence rate for patients with stage I (T1/2 N0) rectal cancer in the range of 4% to 16% at 5 years. There are limited data, however, regarding clinical or pathologic prognostic markers for recurrence in this population.
Objective: The aim of this study is to assess the clinical and pathologic factors associated with local recurrence and overall survival in patients with early-stage rectal cancer after resection.
Design: This is a retrospective study.
Setting: This study was conducted at 2 tertiary care centers in Boston, Massachusetts.
Patients: From 2000 to 2008, 175 patients with stage I rectal cancer treated with local or total mesorectal excision without adjuvant therapy were identified.
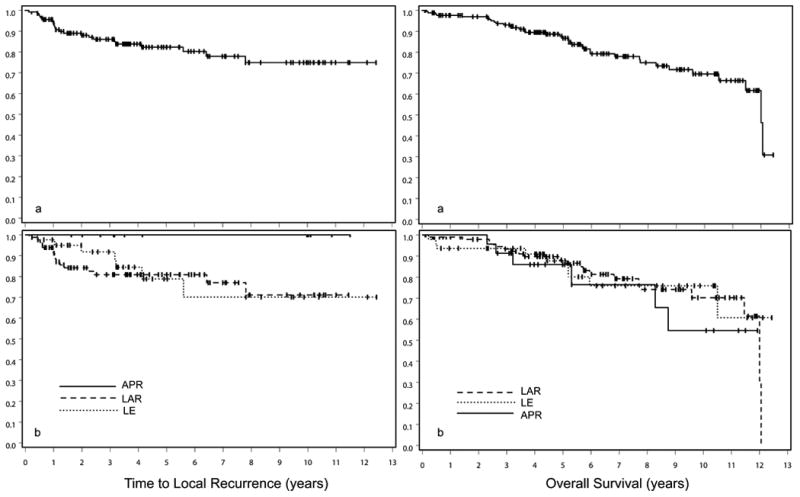
Main outcome measures: Time to local recurrence after resection and overall survival were evaluated for all patients with complete follow-up data. Perioperative data were reviewed to identify staging method, preoperative CEA, type of surgery, tumor size, number of lymph nodes resected, histological grade, circumferential resection margin, perineural invasion, lymphovascular invasion, and tumor ulceration. Data were analyzed by using a Cox proportional hazards regression model.
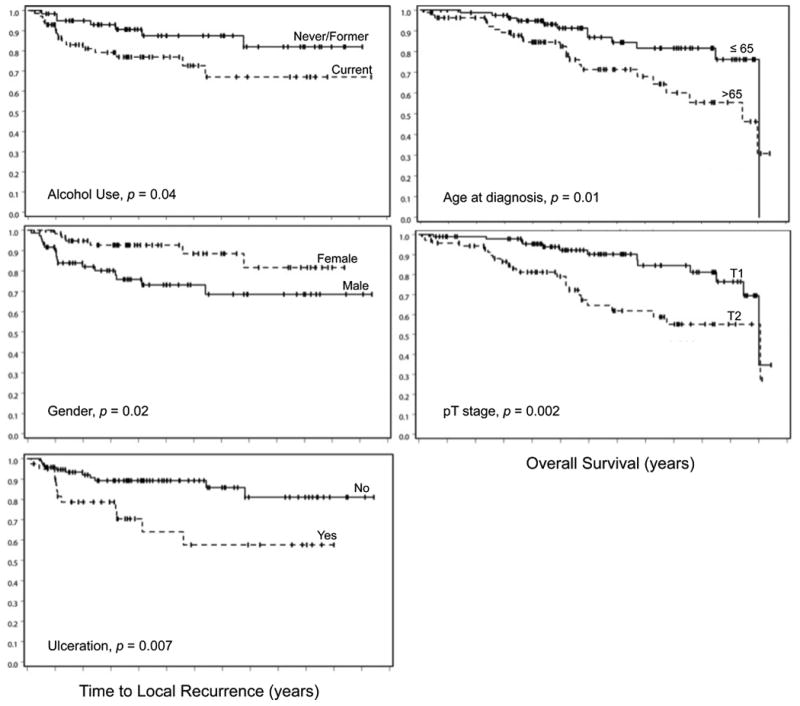
Results: Of the eligible cohort, 137 patients had complete follow-up data for analysis of time to local recurrence, and only 23 (16.8%) patients had local recurrence. Among these 23 patients, the median time to recurrence was 1.1 years (0.1-7.8). On multivariate analysis, male sex, current alcohol use, and tumor ulceration were associated with heightened risk of local recurrence. Of the original cohort, 173 patients had complete follow-up for overall survival analysis. Among these patients, the median overall survival was 12 years. On multivariable analysis, age at diagnosis >65 years and T2 pathologic stage were associated with decreased survival.
Limitations: As in any retrospective study, there is a potential for selection bias. Several patients were excluded from the analysis due to inadequate follow-up data. These results from two academic medical centers with specialized colorectal surgeons may not be generally applicable. The relatively small number of events, ie, recurrences, suggest the findings should be validated in a larger study.
Conclusions: For patients with stage I rectal cancer treated with resection alone, these results provide important prognostic information and may help identify those who could benefit from additional therapy.
Conflict of interest statement
Figures
References
-
- Stamos MJ, Murrell Z. Management of early rectal T1 and T2 cancers. Clin Cancer Res. 2007;13:6885–6889. - PubMed
-
- Blumberg D, Paty PB, Picon AI, et al. Stage I Rectal Cancer: Identification of High-Risk Patients. J Am Coll Surg. 1998;186:574–580. - PubMed
-
- Nagetgaal ID, Marijnen CA, Kranenbarg EK, et al. Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol. 2002;26:350–357. - PubMed
-
- Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
