

Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: a meta-analysis of randomized controlled trials
- PMID: 24610882
- PMCID: PMC4054797
- DOI: 10.1093/ajh/hpu024
Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: a meta-analysis of randomized controlled trials
Abstract
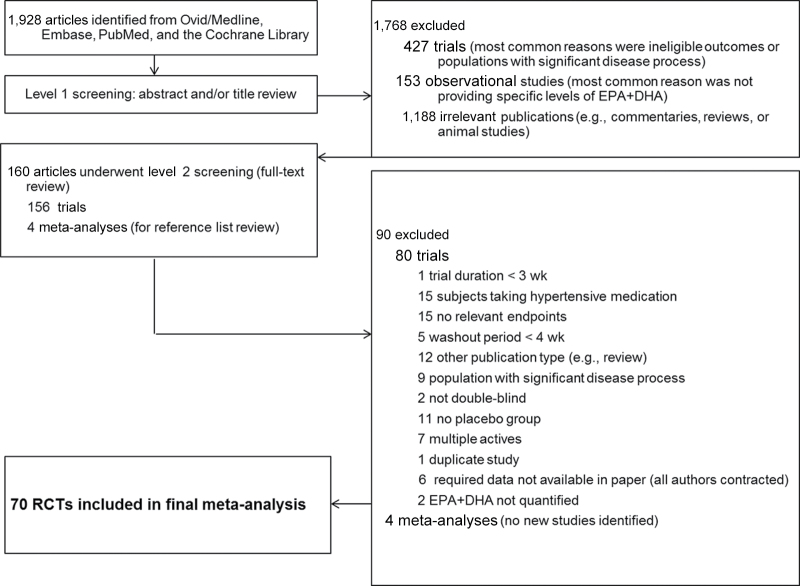
Background: Although a large body of literature has been devoted to examining the relationship between eicosapentaenoic and docosahexaenoic acids (EPA+DHA) and blood pressure, past systematic reviews have been hampered by narrow inclusion criteria and a limited scope of analytical subgroups. In addition, no meta-analysis to date has captured the substantial volume of randomized controlled trials (RCTs) published in the past 2 years. The objective of this meta-analysis was to examine the effect of EPA+DHA, without upper dose limits and including food sources, on blood pressure in RCTs.
Methods: Random-effects meta-analyses were used to generate weighted group mean differences and 95% confidence intervals (CIs) between the EPA+DHA group and the placebo group. Analyses were conducted for subgroups defined by key subject or study characteristics.
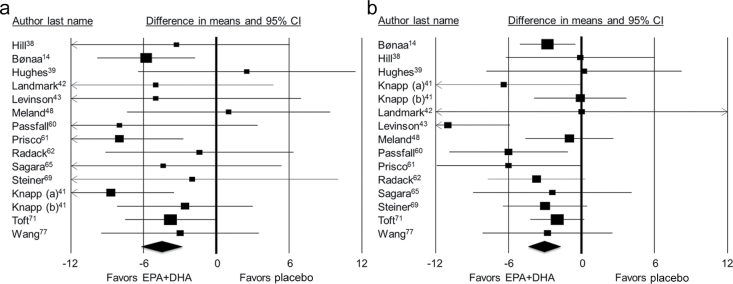
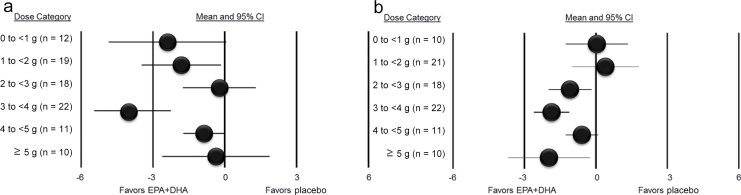
Results: Seventy RCTs were included. Compared with placebo, EPA+DHA provision reduced systolic blood pressure (-1.52 mm Hg; 95% confidence interval (CI) = -2.25 to -0.79) and diastolic blood pressure (-0.99 mm Hg; 95% CI = -1.54 to -0.44) in the meta-analyses of all studies combined. The strongest effects of EPA+DHA were observed among untreated hypertensive subjects (systolic blood pressure = -4.51 mm Hg, 95% CI = -6.12 to -2.83; diastolic blood pressure = -3.05 mm Hg, 95% CI = -4.35 to - 1.74), although blood pressure also was lowered among normotensive subjects (systolic blood pressure = -1.25 mm Hg, 95% CI = -2.05 to -0.46; diastolic blood pressure = -0.62 mm Hg, 95% CI = -1.22 to -0.02).
Conclusions: Overall, available evidence from RCTs indicates that provision of EPA+DHA reduces systolic blood pressure, while provision of ≥2 grams reduces diastolic blood pressure.
Keywords: blood pressure; docosahexaenoic acid; eicosapentaenoic acid; fish oil; hypertension; meta-analysis; omega-3; randomized controlled trials; systematic review.
© The Author 2014. Published by Oxford University Press on behalf of the American Journal of Hypertension.
Figures
References
-
- Centers for Disease Control and Prevention. Vital signs: prevalence, treatment, and control of hypertension—United States, 1999–2002 and 2005–2008. MMWR Morbid Mortal Wkly Rep 2011; 60:103–108. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation 2012; 125:e2–e220. - PMC - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572. - PubMed
-
- Cabo J, Alonso R, Mata P. Omega-3 fatty acids and blood pressure. Br J Nutr 2012; 107:S195–S200. - PubMed
-
- Hartweg J, Farmer AJ, Holman RR, Neil HAW. Meta-analysis of the effects of n-3 polyunsaturated fatty acids on haematological and thrombogenic factors in type 2 diabetes. Diabetologia 2007; 50:250–258. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
