

The role of alexithymia in the development of functional motor symptoms (conversion disorder)
- PMID: 24610939
- PMCID: PMC4173967
- DOI: 10.1136/jnnp-2013-307203
The role of alexithymia in the development of functional motor symptoms (conversion disorder)
Abstract
Background: The mechanisms leading to the development of functional motor symptoms (FMS) are of pathophysiological and clinical relevance, yet are poorly understood.
Aim: The aim of the present study was to evaluate whether impaired emotional processing at the cognitive level (alexithymia) is present in patients affected by FMS. We conducted a cross-sectional study in a population of patients with FMS and in two control groups (patients with organic movement disorders (OMD) and healthy volunteers).
Methods: 55 patients with FMS, 33 patients affected by OMD and 34 healthy volunteers were recruited. The assessment included the 20-item Toronto Alexithymia Scale (TAS-20), the Montgomery-Asberg Depression Rating Scale, the Reading the Mind in the Eyes' Test and the Structured Clinical Interview for Personality Disorders.
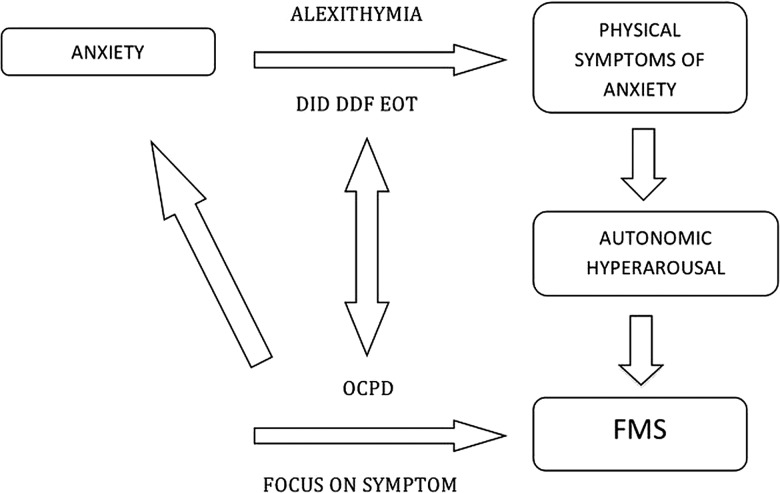
Results: Alexithymia was present in 34.5% of patients with FMS, 9.1% with OMD and 5.9% of the healthy volunteers, which was significantly higher in the FMS group (χ(2) (2)=14.129, p<0.001), even after controlling for the severity of symptoms of depression. Group differences in mean scores were observed on both the difficulty identifying feelings and difficulty describing feelings dimensions of the TAS-20, whereas the externally orientated thinking subscale score was similar across the three groups. Regarding personality disorder, χ(2) analysis showed a significantly higher prominence of obsessive-compulsive personality disorder (OCPD) in the FMS group (χ(2) (2)=16.217, p<0.001) and 71.4% of those with OCPD also reached threshold criteria for alexithymia.
Conclusions: Because alexithymia is a mental state denoting the inability to identify emotions at a cognitive level, one hypothesis is that some patients misattribute autonomic symptoms of anxiety, for example, tremor, paraesthesiae, paralysis, to that of a physical illness. Further work is required to understand the contribution of OCPD to the development of FMS.
Keywords: NEUROPSYCHIATRY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Stone J, Carson A, Duncan R, et al. Who is referred to neurology clinics?—the diagnoses made in 3781 new patients. Clin Neurol Neurosurg 2010;112:747–51 - PubMed
-
- Carson A, Stone J, Hibberd C, et al. Disability, distress and unemployment in neurology outpatients with symptoms “unexplained by organic disease”. J Neurol Neurosurg Psychiatry 2011;82:810–13 - PubMed
-
- Roelofs K, Spinhoven P. Trauma and medically unexplained symptoms towards an integration of cognitive and neuro-biological accounts. Clin Psychol Rev 2007;27:798–820 - PubMed
-
- Sharpe D, Faye C. Non-epileptic seizures and child sexual abuse: a critical review of the literature. Clin Psychol Rev 2006;26:1020–40 - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-V). 5th edn. Washington, DC: American Psychiatric Press, 2013
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous