

Effectiveness of a community-based intervention for people with schizophrenia and their caregivers in India (COPSI): a randomised controlled trial
- PMID: 24612754
- PMCID: PMC4255067
- DOI: 10.1016/S0140-6736(13)62629-X
Effectiveness of a community-based intervention for people with schizophrenia and their caregivers in India (COPSI): a randomised controlled trial
Erratum in
- Lancet. 2014 Jun 14;383(9934):2046
Abstract
Background: Observational evidence suggests that community-based services for people with schizophrenia can be successfully provided by community health workers, when supervised by specialists, in low-income and middle-income countries. We did the COmmunity care for People with Schizophrenia in India (COPSI) trial to compare the effectiveness of a collaborative community-based care intervention with standard facility-based care.
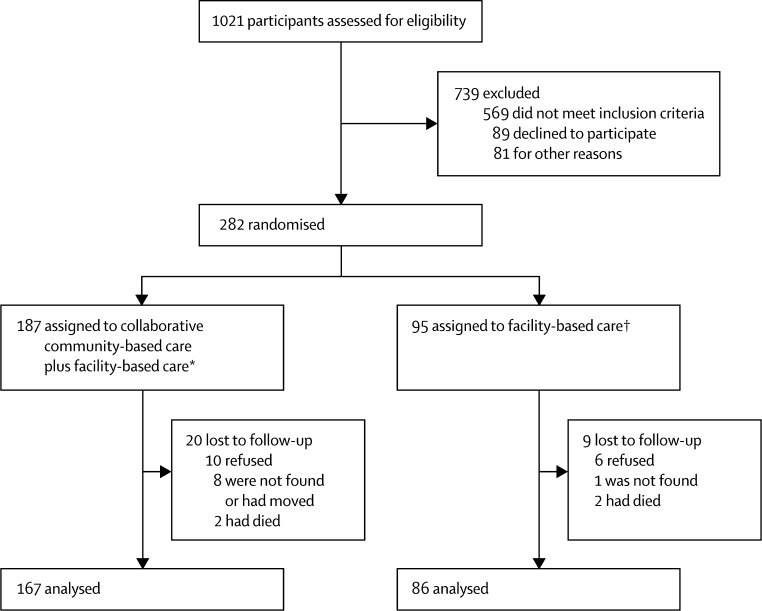
Methods: We did a multicentre, parallel-group, randomised controlled trial at three sites in India between Jan 1, 2009 and Dec 31, 2010. Patients aged 16-60 years with a primary diagnosis of schizophrenia according to the tenth edition of the International Classification of Diseases, Diagnostic Criteria for Research (ICD-10-DCR) were randomly assigned (2:1), via a computer-generated randomisation list with block sizes of three, six, or nine, to receive either collaborative community-based care plus facility-based care or facility-based care alone. Randomisation was stratified by study site. Outcome assessors were masked to group allocation. The primary outcome was a change in symptoms and disabilities over 12 months, as measured by the positive and negative syndrome scale (PANSS) and the Indian disability evaluation and assessment scale (IDEAS). Analysis was by modified intention to treat. This study is registered as an International Standard Randomised Controlled Trial, number ISRCTN 56877013.
Findings: 187 participants were randomised to the collaborative community-based care plus facility-based care group and 95 were randomised to the facility-based care alone group; 253 (90%) participants completed follow-up to month 12. At 12 months, total PANSS and IDEAS scores were lower in patients in the intervention group than in those in the control group (PANSS adjusted mean difference -3.75, 95% CI -7.92 to 0.42; p=0.08; IDEAS -0.95, -1.68 to -0.23; p=0.01). However, no difference was shown in the proportion of participants who had a reduction of more than 20% in overall symptoms (PANSS 85 [51%] in the intervention group vs 44 [51%] in the control group; p=0.89; IDEAS 75 [48%] vs 28 [35%]). We noted a significant reduction in symptom and disability outcomes at the rural Tamil Nadu site (-9.29, -15.41 to -3.17; p=0.003). Two patients (one in each group) died by suicide during the study, and two patients died because of complications of a road traffic accident and pre-existing cardiac disease. 18 (73%) patients (17 in the intervention group) were admitted to hospital during the course of the trial, of whom seven were admitted because of physical health problems, such as acute gastritis and vomiting, road accident, high fever, or cardiovascular disease.
Interpretation: The collaborative community-based care plus facility-based care intervention is modestly more effective than facility-based care, especially for reducing disability and symptoms of psychosis. Our results show that the study intervention is best implemented as an initial service in settings where services are scarce, for example in rural areas.
Funding: Wellcome Trust.
Copyright © 2014 Chatterjee et al. Open Access article distributed under the terms of CC BY-NC-ND. Published by Elsevier Ltd. All rights reserved.
Comment in
-
Community based treatment for schizophrenia is effective in low income countries.BMJ. 2014 Mar 6;348:g1984. doi: 10.1136/bmj.g1984. BMJ. 2014. PMID: 24603959 No abstract available.
-
Challenges in rolling out interventions for schizophrenia.Lancet. 2014 Apr 19;383(9926):1362-4. doi: 10.1016/S0140-6736(14)60085-4. Epub 2014 Mar 5. Lancet. 2014. PMID: 24612753 No abstract available.
-
Interventions for people with schizophrenia and their caregivers in India.Lancet. 2014 Jul 19;384(9939):231. doi: 10.1016/S0140-6736(14)61206-X. Lancet. 2014. PMID: 25042228 No abstract available.
-
Interventions for people with schizophrenia and their caregivers in India--authors' reply.Lancet. 2014 Jul 19;384(9939):231-2. doi: 10.1016/S0140-6736(14)61207-1. Lancet. 2014. PMID: 25042229 No abstract available.
-
Community-based intervention for people with schizophrenia successfully provided by supervised community health workers in a low-resource setting.Evid Based Ment Health. 2014 Nov;17(4):124. doi: 10.1136/eb-2014-101893. Epub 2014 Sep 19. Evid Based Ment Health. 2014. PMID: 25239250 No abstract available.
-
The COPSI Trial: additional fidelity testing needed.Lancet. 2014 Nov 1;384(9954):1572-3. doi: 10.1016/S0140-6736(14)61979-6. Epub 2014 Oct 31. Lancet. 2014. PMID: 25443482 No abstract available.
-
The COPSI Trial: additional fidelity testing needed - Authors' reply.Lancet. 2014 Nov 1;384(9954):1573-4. doi: 10.1016/S0140-6736(14)61980-2. Epub 2014 Oct 31. Lancet. 2014. PMID: 25443484 No abstract available.
References
-
- Lund C, De Silva M, Plagerson S. Poverty and mental disorders: breaking the cycle in low-income and middle-income countries. Lancet. 2011;378:1502–1514. - PubMed
-
- Thornicroft G, Brohan E, Rose D, Sartorius N, Leese M, the INDIGO Study Group Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey. Lancet. 2009;373:408–415. - PubMed
Uncited Reference
-
- Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, the CONSORT Group Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Ann Intern Med. 2008;148:295–309. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
