

Mindfulness-based cognitive therapy (MBCT) versus the health-enhancement program (HEP) for adults with treatment-resistant depression: a randomized control trial study protocol
- PMID: 24612825
- PMCID: PMC3995768
- DOI: 10.1186/1472-6882-14-95
Mindfulness-based cognitive therapy (MBCT) versus the health-enhancement program (HEP) for adults with treatment-resistant depression: a randomized control trial study protocol
Abstract
Background: Major depressive disorder (MDD) is the leading cause of disability in the developed world, yet broadly effective treatments remain elusive. Up to 40% of patients with depression are unresponsive to at least two trials of antidepressant medication and thus have "treatment-resistant depression" (TRD). There is an urgent need for cost-effective, non-pharmacologic, evidence-based treatments for TRD. Mindfulness-Based Cognitive Therapy (MBCT) is an effective treatment for relapse prevention and residual depression in major depression, but has not been previously studied in patients with TRD in a large randomized trial.
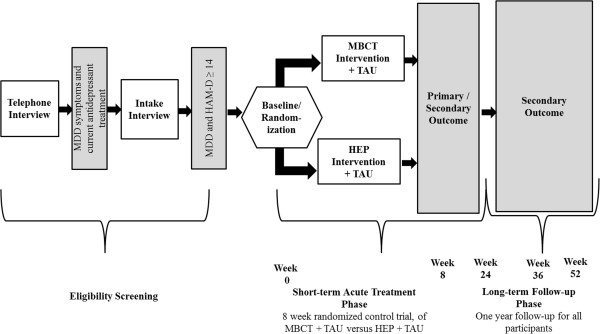
Methods/design: The purpose of this study was to evaluate whether MBCT is an effective augmentation of antidepressants for adults with MDD who failed to respond to standard pharmacotherapy. MBCT was compared to an active control condition, the Health-Enhancement Program (HEP), which incorporates physical activity, functional movement, music therapy and nutritional advice. HEP was designed as a comparator condition for mindfulness-based interventions to control for non-specific effects. Originally investigated in a non-clinical sample to promote stress reduction, HEP was adapted for a depressed population for this study. Individuals age 18 and older with moderate to severe TRD, who failed to respond to at least two trials of antidepressants in the current episode, were recruited to participate. All participants were taking antidepressants (Treatment as usual; TAU) at the time of enrollment. After signing an informed consent, participants were randomly assigned to either MBCT or HEP condition. Participants were followed for 1 year and assessed at weeks 1-7, 8, 24, 36, and 52. Change in depression severity, rate of treatment response and remission after 8 weeks were the primary outcomes measured by the clinician-rated Hamilton Depression Severity Rating (HAM-D) 17-item scale. The participant-rated Quick Inventory of Depression Symptomology (QIDS-SR) 16-item scale was the secondary outcome measure of depression severity, response, and remission.
Discussion: Treatment-resistant depression entails significant morbidity and has few effective treatments. We studied the effect of augmenting antidepressant medication with MBCT, compared with a HEP control, for patients with TRD. Analyses will focus on clinician and patient assessment of depression, participants' clinical global impression change, employment and social functioning scores and quality of life and satisfaction ratings.
Trial registration: ClincalTrials.gov identifier: NCT01021254.
Figures
References
-
- Health M, editor. Volume The WHO Report 2001: Menatl Health, New Understanding, New Hope. New Hope: WHO; 2001. Burden of mental and behavioral disorders.
-
- Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, Ritz L, Biggs MM, Warden D, Luther JF, Shores-Wilson K, Niederehe G, Fava M. STAR*D Study Team. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med. 2006;354(12):1231–1242. doi: 10.1056/NEJMoa052963. - DOI - PubMed
-
- Greden JF. The burden of disease for treatment-resistant depression. J Clin Psychiatry. 2001;62(Suppl 16):26–31. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
