

Computerized self-interviews improve Chlamydia and gonorrhea testing among youth in the emergency department
- PMID: 24612901
- PMCID: PMC4156563
- DOI: 10.1016/j.annemergmed.2014.01.031
Computerized self-interviews improve Chlamydia and gonorrhea testing among youth in the emergency department
Abstract
Study objective: National guidelines recommend annual Chlamydia trachomatis and Neisseria gonorrhoeae screening for sexually active youth at risk for infection. These infections have serious sequelae in women if untreated, and methods to improve testing are needed. We hypothesize that an electronic method of identifying at-risk youth will significantly increase testing for these sexually transmitted infections during emergency department (ED) visits.
Methods: We developed an audio-enhanced computer-assisted self-interview (ACASI) to obtain sexual histories from ED patients and an embedded decision tree to create a sexually transmitted infection testing recommendation. ED health care providers were prompted by the electronic medical record to review the participant answers and testing recommendations, and to offer testing to at-risk youth. Patients aged 15 to 21 years and visiting the St. Louis Children's Hospital ED, regardless of complaint, were eligible for participation.
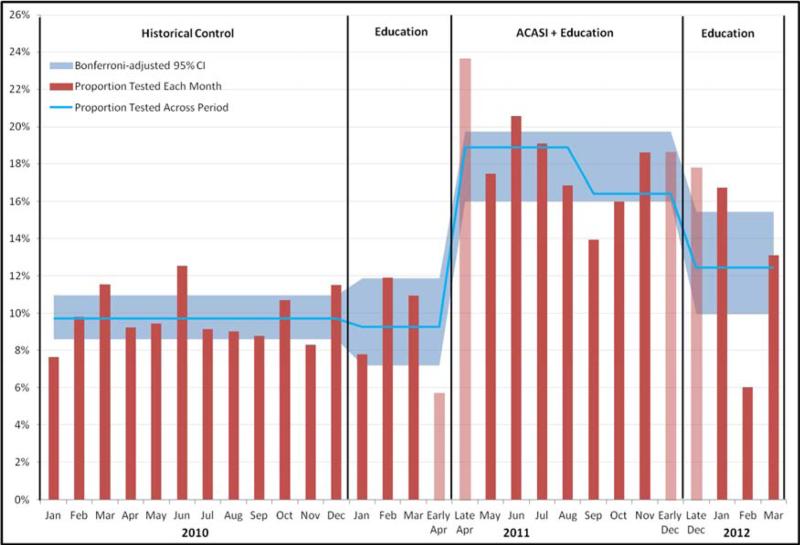
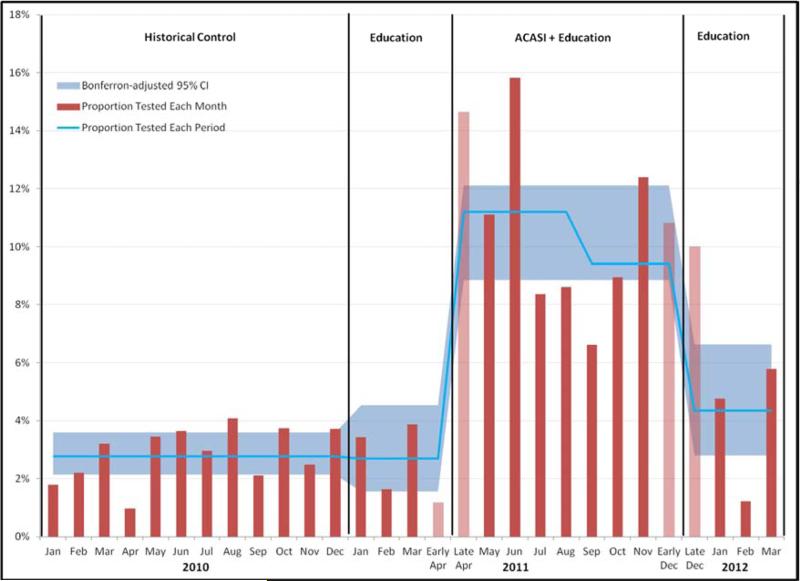
Results: Sexually transmitted infection testing among all 15- to 21-year-old ED patients increased from 9.3% in the 3 months before the ACASI to 17.8% during the 8-month period the ACASI was available and diminished to 12.4% in the 3 months after ACASI withdrawal (P<.001). During the ACASI period, we approached 51.4% of eligible patients and enrolled 59.8% (800/1,337) of those approached. Among ACASI participants, 52.4% (419/800) received a recommendation to receive sexually transmitted infection testing. Of these patients, 52.7% (221/419) received testing in the ED and 18.1% (40/221) of those tested had positive results for chlamydia or gonorrhea, 55% of whom (22/40) had chief complaints unrelated to sexually transmitted infections. Most participants (89%) rated the ACASI easy to use.
Conclusion: Sexually transmitted infection testing in the ED significantly increased during ACASI use and diminished after withdrawal. The ACASI was well accepted by youth and holds promise for enhancing sexually transmitted infection testing in the ED.
Copyright © 2014 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Centers for Disease Control and Prevention . Sexually Transmitted Disease Surveillance 2010. Department of Health and Human Services; 2011.
-
- Centers for Disease Control and Prevention Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010 Dec 17;59(RR-12):1–110. - PubMed
-
- Centers for Disease Control and Prevention Chlamydia screening among sexually active young female enrollees of health plans--United States, 2000-2007. MMWR Morb Mortal Wkly Rep. 2009 Apr 17;58(14):362–365. - PubMed
-
- Bureau of HIV, STD, and Hepatitis Division of Community and Public Health. Missouri Department of Health and Senior Services. 2010 Epidemiologic Profiles of HIV, STD, and Hepatitis in Missouri. 2011
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
