

Transient lesion in the splenium of the corpus callosum in acute uncomplicated falciparum malaria
- PMID: 24615139
- PMCID: PMC4047739
- DOI: 10.4269/ajtmh.13-0665
Transient lesion in the splenium of the corpus callosum in acute uncomplicated falciparum malaria
Abstract
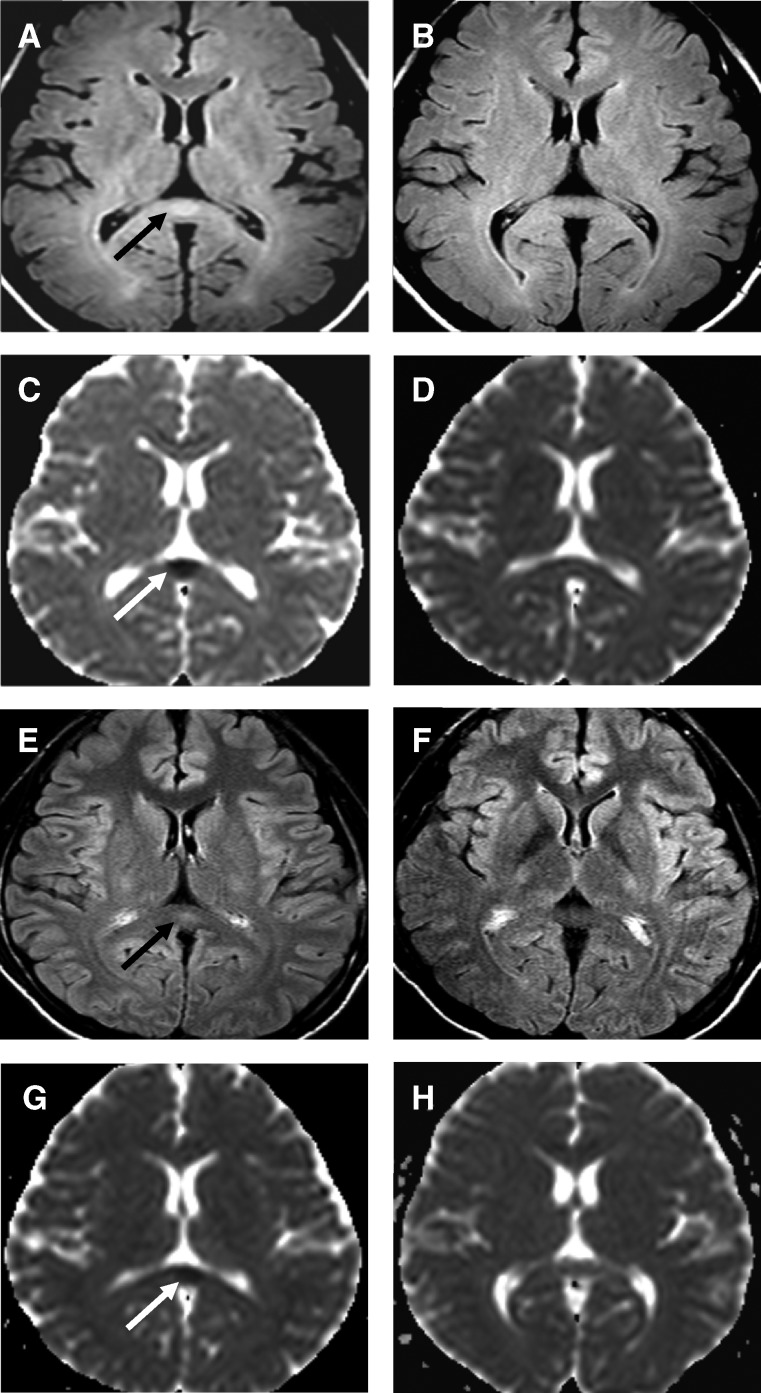
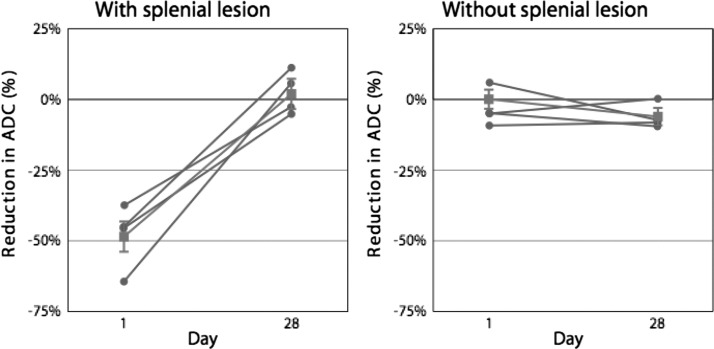
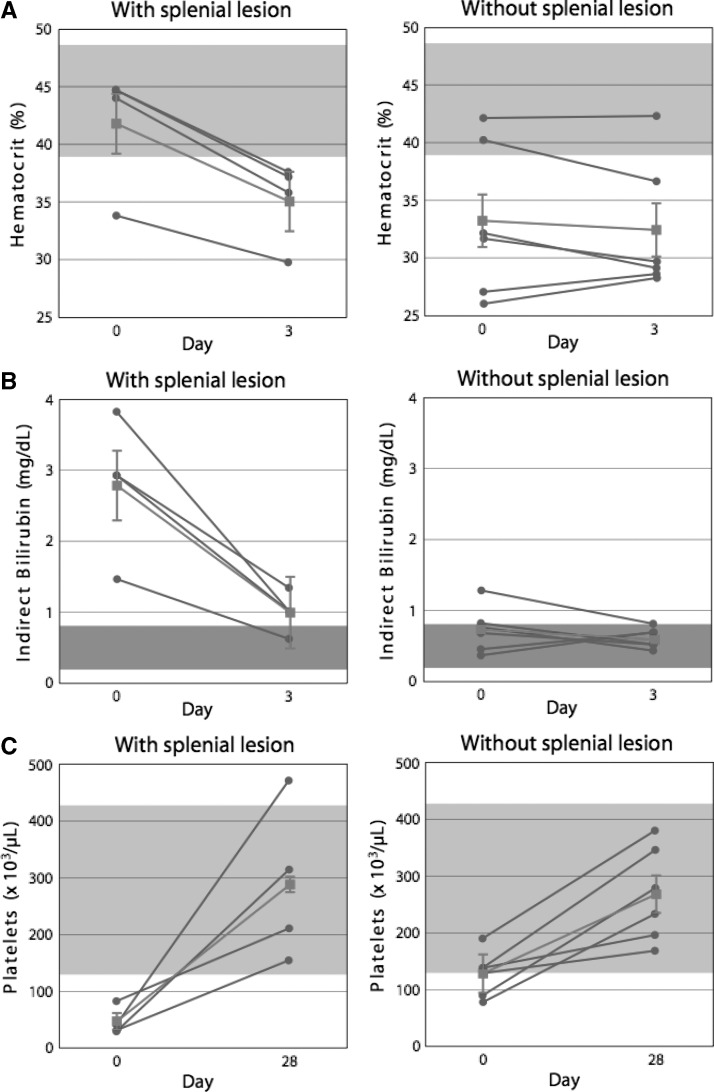
Patients with acute uncomplicated Plasmodium falciparum malaria have no evident neurologic disorder, vital organ dysfunction, or other severe manifestations of infection. Nonetheless, parasitized erythrocytes cytoadhere to the endothelium throughout their microvasculature, especially within the brain. We aimed to determine if 3 Tesla magnetic resonance imaging studies could detect evidence of cerebral abnormalities in these patients. Within 24 hours of admission, initial magnetic resonance imaging examinations found a lesion with restricted water diffusion in the mid-portion of the splenium of the corpus callosum of 4 (40%) of 10 male patients. The four patients who had a splenial lesion initially had evidence of more severe hemolysis and thrombocytopenia than the six patients who had no apparent abnormality. Repeat studies four weeks later found no residua of the lesions and resolution of the hematologic differences. These observations provide evidence for acute cerebral injury in the absence of severe or cerebral malaria.
© The American Society of Tropical Medicine and Hygiene.
Figures
References
-
- Pongponratn E, Turner GD, Day NP, Phu NH, Simpson JA, Stepniewska K, Mai NT, Viriyavejakul P, Looareesuwan S, Hien TT, Ferguson DJ, White NJ. An ultrastructural study of the brain in fatal Plasmodium falciparum malaria. Am J Trop Med Hyg. 2003;69:345–359. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
