

External fixation for closed pediatric femoral shaft fractures: where are we now?
- PMID: 24615424
- PMCID: PMC4397747
- DOI: 10.1007/s11999-014-3554-5
External fixation for closed pediatric femoral shaft fractures: where are we now?
Abstract
Background: Recent advances in external fixation technique and pin design have sought to minimize complications such as pin site infection and premature removal of the external fixator. Although newer forms of internal fixation have gained popularity, external fixation may still have a role in managing pediatric femoral shaft fractures.
Questions/purposes: We sought to assess the time to healing, limb alignment, and complications observed in a cohort of pediatric patients with closed femoral shaft fractures who were treated with external fixation.
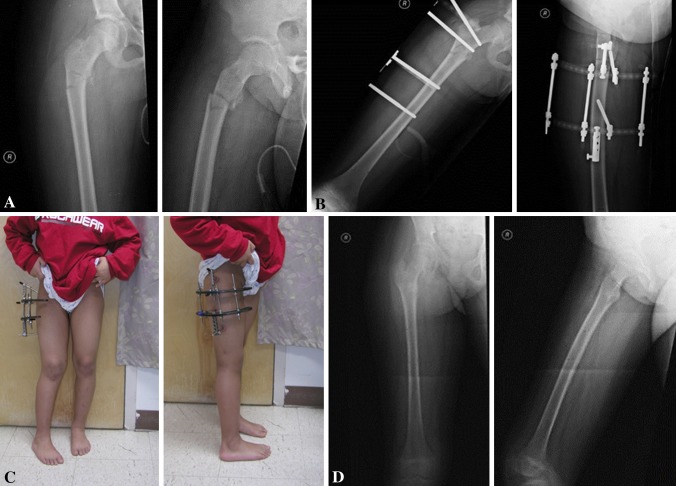
Methods: Over a 15-year period, one surgeon treated 289 pediatric patients with femur fractures, 31 (11%) of whom received an external fixator. The general indications for use of an external fixator during the period in question included length-unstable fractures, metadiaphyseal location, refracture, and pathologic fracture. Six patients (19%) had inadequate followup data and four patients (13%) were treated with a combination of flexible intramedullary nails and external fixation, leaving 21 patients for analysis. Mean age at injury was 10 years (range, 6-15 years) and followup averaged 22 months (range, 5-45 months) after removal of the fixator. Radiographs were examined for alignment and limb length discrepancy. Complications were recorded from a chart review.
Results: Mean time in the fixator was 17 weeks (range, 9-24 weeks). One patient sustained a refracture and one patient with an isolated femur fracture had a leg length discrepancy > 2 cm. There were no pin site infections requiring intravenous antibiotics or additional surgery. One patient with Blount disease and previous tibial osteotomy developed transient peroneal nerve palsy.
Conclusions: Despite improvements in pin design and predictable fracture healing, complications such as refracture and leg length discrepancy after external fixation of pediatric femoral shaft fractures can occur. However, external fixation remains a viable alternative for certain fractures such as length-unstable fractures, metadiaphyseal location, pathologic fractures, and refractures.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
