

Brain injury in premature neonates: A primary cerebral dysmaturation disorder?
- PMID: 24615937
- PMCID: PMC5989572
- DOI: 10.1002/ana.24132
Brain injury in premature neonates: A primary cerebral dysmaturation disorder?
Abstract
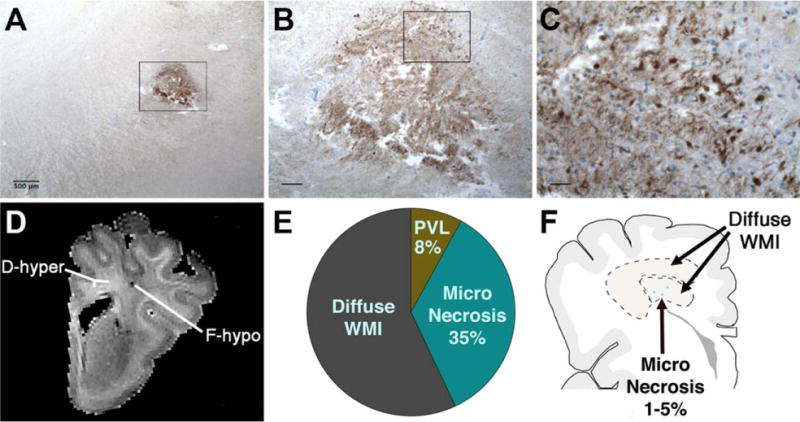
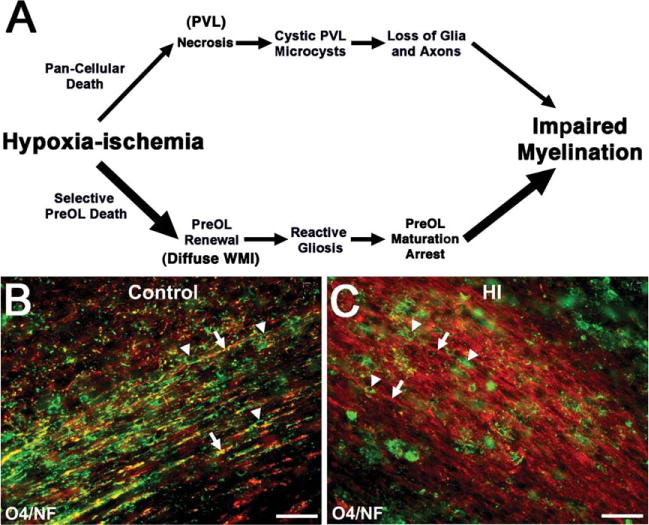
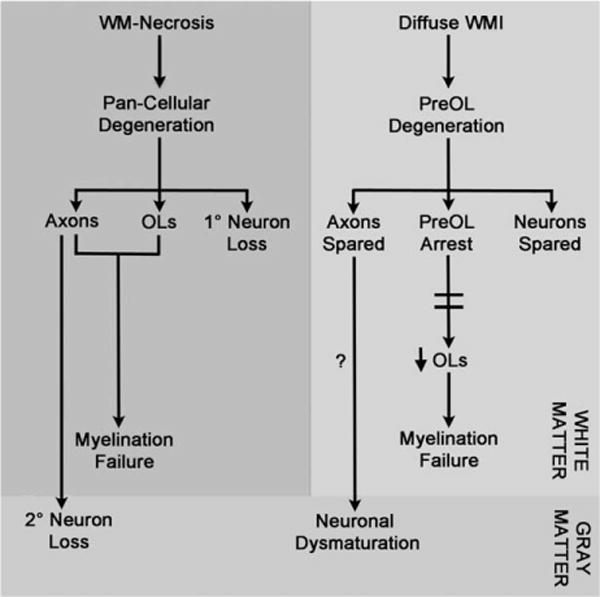
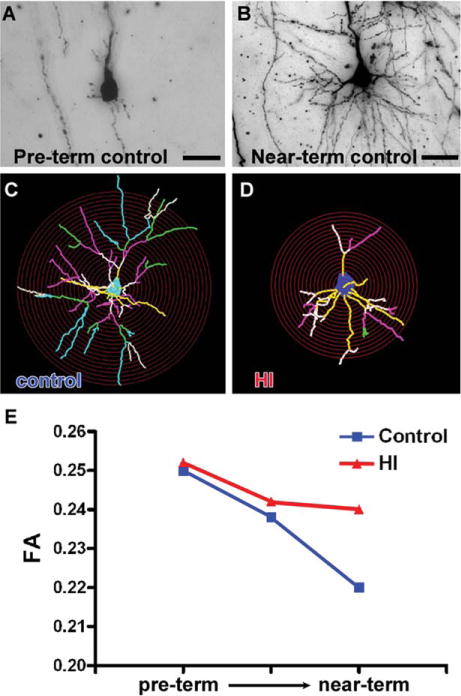
With advances in neonatal care, preterm neonates are surviving with an evolving constellation of motor and cognitive disabilities that appear to be related to widespread cellular maturational disturbances that target cerebral gray and white matter. Whereas preterm infants were previously at high risk for destructive brain lesions that resulted in cystic white matter injury and secondary cortical and subcortical gray matter degeneration, contemporary cohorts of preterm survivors commonly display less severe injury that does not appear to involve pronounced glial or neuronal loss. Nevertheless, these milder forms of injury are also associated with reduced cerebral growth. Recent human and experimental studies support that impaired cerebral growth is related to disparate responses in gray and white matter. Myelination disturbances in cerebral white matter are related to aberrant regeneration and repair responses to acute death of premyelinating late oligodendrocyte progenitors (preOLs). In response to preOL death, early oligodendrocyte progenitors rapidly proliferate and differentiate, but the regenerated preOLs fail to normally mature to myelinating cells required for white matter growth. Although immature neurons appear to be more resistant to cell death from hypoxia-ischemia than glia, they display widespread disturbances in maturation of their dendritic arbors, which further contribute to impaired cerebral growth. These complex and disparate responses of neurons and preOLs thus result in large numbers of cells that fail to fully mature during a critical window in development of neural circuitry. These recently recognized forms of cerebral gray and white matter dysmaturation raise new diagnostic challenges and suggest new therapeutic directions centered on reversal of the processes that promote dysmaturation.
© 2014 American Neurological Association.
Conflict of interest statement
Nothing to report.
Figures
References
-
- March of Dimes. Prematurity campaign. Available at: http://www.marchofdimes.com/mission/prematurity-campaign.aspx. Accessed on March 19, 2014.
-
- Synnes AR, Anson S, Arkesteijn A, et al. School entry age outcomes for infants with birth weight 800 grams. J Pediatr. 2010;157:989–994. - PubMed
-
- Miller SP, Ferriero DM, Leonard C, et al. Early brain injury in premature newborns detected with magnetic resonance imaging is associated with adverse early neurodevelopmental outcome. J Pediatr. 2005;147:609–616. - PubMed
-
- Vohr BR, Allan WC, Westerveld M, et al. School-age outcomes of very low birth weight infants in the indomethacin intraventricular hemorrhage prevention trial. Pediatrics. 2003;111:e340–e346. - PubMed
-
- Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic and developmental disability at six years of age after extremely preterm birth. N Engl J Med. 2005;352:9–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
