

HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. Veterans with HCV
- PMID: 24615981
- PMCID: PMC4689301
- DOI: 10.1002/hep.27095
HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. Veterans with HCV
Abstract
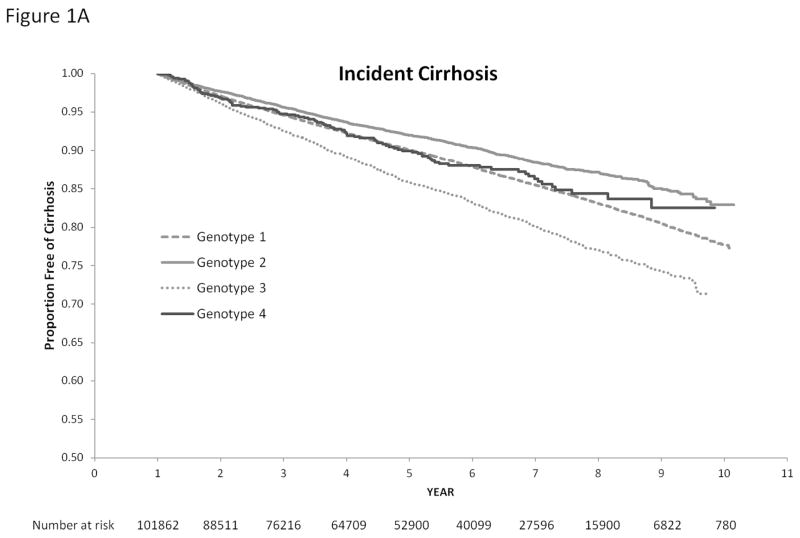
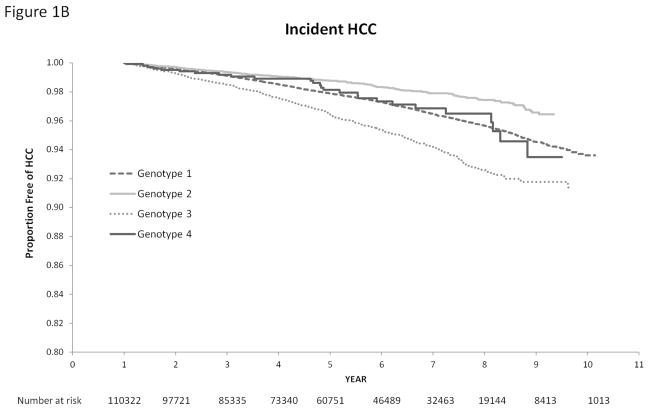
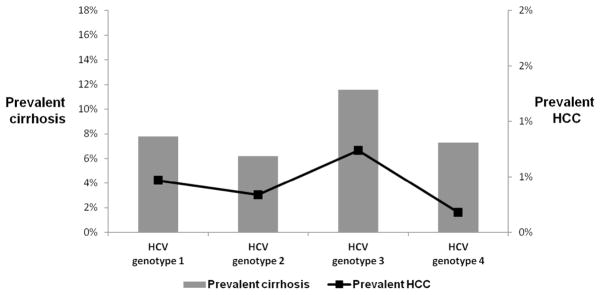
Data show that viral genotype 1 may increase the risk of cirrhosis and hepatocellular carcinoma (HCC) compared to genotype 2 in patients with chronic hepatitis C virus (HCV) infection. However, the effect of HCV genotype 3 on cirrhosis and HCC risk is uncertain. We identified patients with active HCV infection, confirmed by positive polymerase chain reaction (PCR) and a known HCV genotype, from the VA HCV Clinical Case Registry between 2000 and 2009. We examined the effect of HCV genotype on the risk of cirrhosis and HCC in a Cox proportional hazards model adjusting for patients' age, period of service (World War I/II, Vietnam era, post-Vietnam era), race, gender, human immunodeficiency virus (HIV) infection, alcohol use, diabetes, body mass index, and antiviral treatment receipt. Of the 110,484 patients with active HCV viremia, 88,348 (79.9%) had genotype 1, 13,077 (11.8%) genotype 2, 8,337 (7.5%) genotype 3, and 1,082 (0.9%) patients had genotype 4 infection. Despite being younger, patients with genotype 3 had a higher risk of developing cirrhosis (unadjusted hazard ratio [HR] = 1.40, 95% confidence interval [CI] = 1.32-1.50) and HCC (unadjusted HR = 1.66, 95% CI = 1.48-1.85) than HCV genotype 1 patients. After adjustment for prespecified demographic, clinical, and antiviral treatment factors, the risk of cirrhosis and HCC was 31% (adjusted HR = 1.31, 95% CI = 1.22-1.39) and 80% (adjusted HR = 1.80, 95% CI = 1.61-2.03) higher in patients with genotype 3 compared to genotype 1 infected patients.
Conclusion: HCV genotype 3 is associated with a significantly increased risk of developing cirrhosis and HCC compared to HCV genotype 1. This association is independent of patients' age, diabetes, body mass index, or antiviral treatment.
© 2014 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
References
-
- Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006 May 16;144(10):705–714. - PubMed
-
- Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010 Feb;138(2):513–21. 521. - PubMed
-
- Kanwal F, Kramer J, Asch SM, El-Serag H, Spiegel BM, Edmundowicz S, et al. An explicit quality indicator set for measurement of quality of care in patients with cirrhosis. Clin Gastroenterol Hepatol. 2010 Aug;8(8):709–717. - PubMed
-
- Missiha SB, Ostrowski M, Heathcote EJ. Disease progression in chronic hepatitis C: modifiable and nonmodifiable factors. Gastroenterology. 2008 May;134(6):1699–1714. - PubMed
-
- Seeff LB. Natural history of chronic hepatitis C. Hepatology. 2002 Nov;36(5 Suppl 1):S35–S46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical