

Effect of the pretransplant serum sodium concentration on outcomes following liver transplantation
- PMID: 24616214
- PMCID: PMC4128788
- DOI: 10.1002/lt.23860
Effect of the pretransplant serum sodium concentration on outcomes following liver transplantation
Abstract
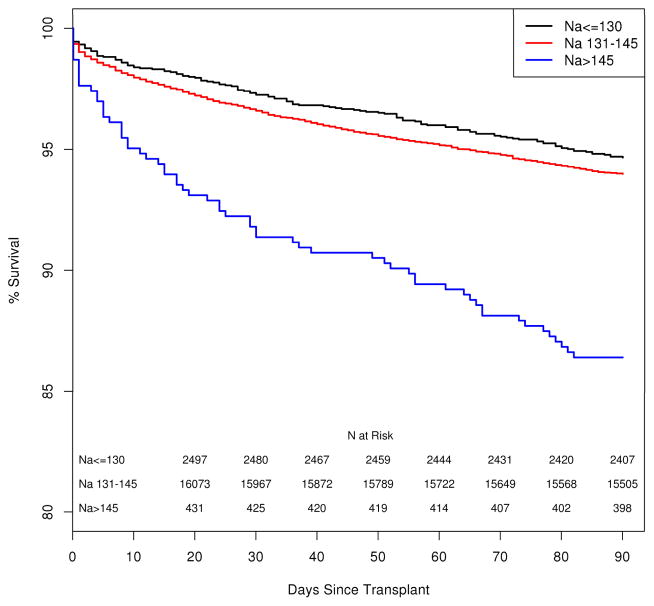
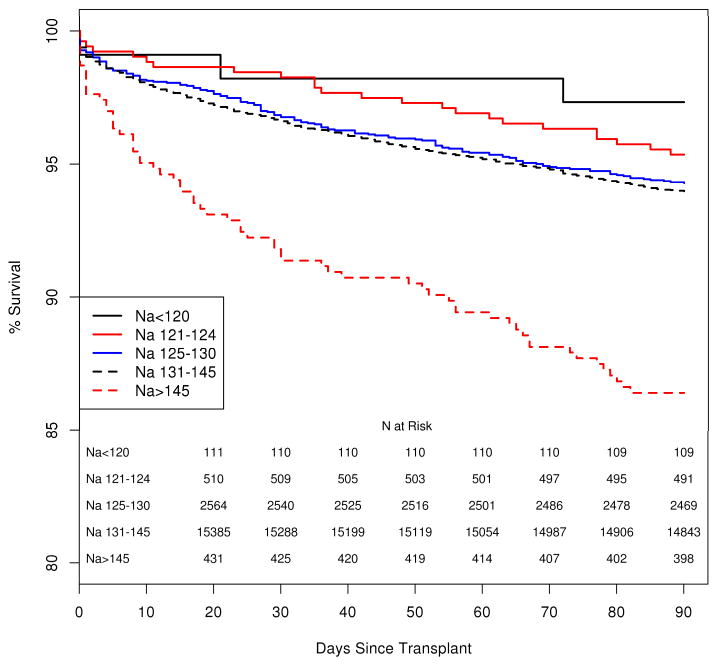
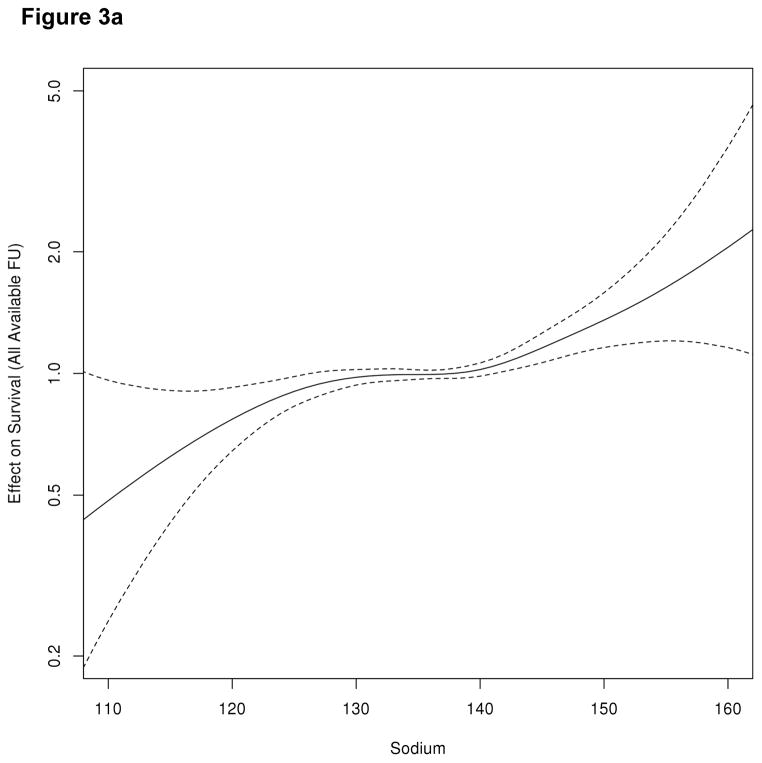
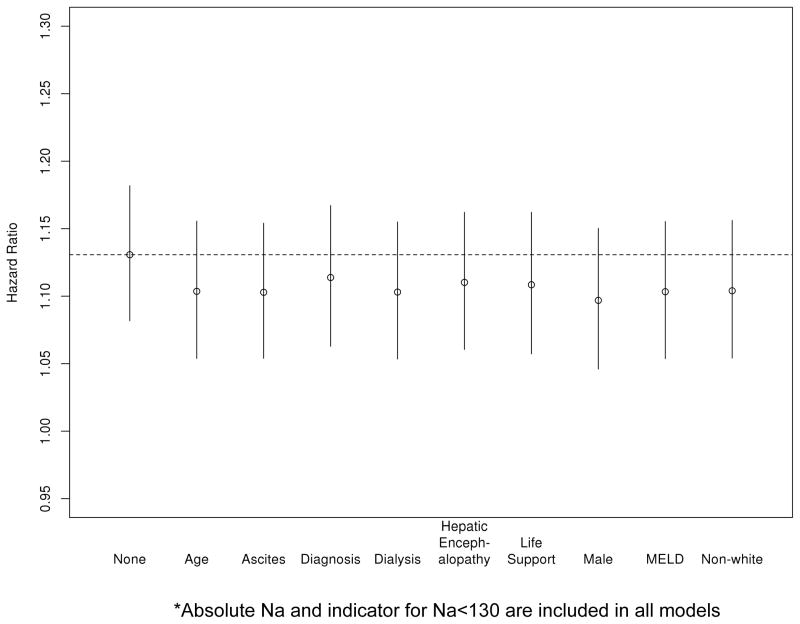
Hyponatremia is associated with an increased risk of mortality on the liver transplantation (LT) waiting list. Although the incorporation of the serum sodium (Na) level into the Model for End-Stage Liver Disease score may reduce wait-list mortality, concerns remain about a potential association between pre-LT hyponatremia and decreased post-LT survival. Furthermore, the relationship between pre-LT hypernatremia and post-LT survival remains unexplored. The purpose of this study was to investigate the impact of the entire spectrum of pre-LT serum Na levels on post-LT outcomes. We identified 19,537 patients from 2003 to 2010 for whom serum Na levels immediately before LT were available. The patients were divided into 3 groups [hyponatremic (Na ≤ 130 mEq/L), normonatremic (Na = 131-145 mEq/L), and hypernatremic (Na > 145 mEq/L)], and their post-LT outcomes were compared. There was no difference in in-hospital mortality or 90-day survival between patients with hyponatremia and patients with normonatremia. A fraction of the patients (2.4%) had hypernatremia, which was associated with increased in-hospital mortality (11.2% versus 4.2%, P < 0.001) and diminished 90-day survival (86.4% versus 94.0.%, P < 0.001). After adjustments for important clinical variables, the association of pre-LT hypernatremia with posttransplant mortality remained significant with a hazard ratio of 1.13 for each unit increase in the Na level > 145 mEq/L (P < 0.001). The duration of the hospitalization after LT was significantly longer for hypernatremic patients (P < 0.001). In conclusion, hyponatremia per se does not affect post-LT survival. Pre-LT hypernatremia is a highly significant risk factor for post-LT mortality.
© 2014 American Association for the Study of Liver Diseases.
Figures

References
-
- Gines A, Escorsell A, Gines P, Salo J, Jimenez W, Inglada L, et al. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology. 1993;105(1):229–36. - PubMed
-
- Gines P, Berl T, Bernardi M, Bichet DG, Hamon G, Jimenez W, et al. Hyponatremia in cirrhosis: from pathogenesis to treatment. Hepatology. 1998;28(3):851–64. - PubMed
-
- Ruf AE, Kremers WK, Chavez LL, Descalzi VI, Podesta LG, Villamil FG. Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone. Liver Transpl. 2005;11(3):336–43. - PubMed
-
- Follo A, Llovet JM, Navasa M, Planas R, Forns X, Francitorra A, et al. Renal impairment after spontaneous bacterial peritonitis in cirrhosis: incidence, clinical course, predictive factors and prognosis. Hepatology. 1994;20(6):1495–501. - PubMed
-
- Guevara M, Baccaro ME, Torre A, Gomez-Anson B, Rios J, Torres F, et al. Hyponatremia is a risk factor of hepatic encephalopathy in patients with cirrhosis: a prospective study with time-dependent analysis. Am J Gastroenterol. 2009;104(6):1382–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources