

Long-term results of reconstruction with pelvic allografts after wide resection of pelvic sarcomas
- PMID: 24616637
- PMCID: PMC3925599
- DOI: 10.1155/2014/605019
Long-term results of reconstruction with pelvic allografts after wide resection of pelvic sarcomas
Abstract
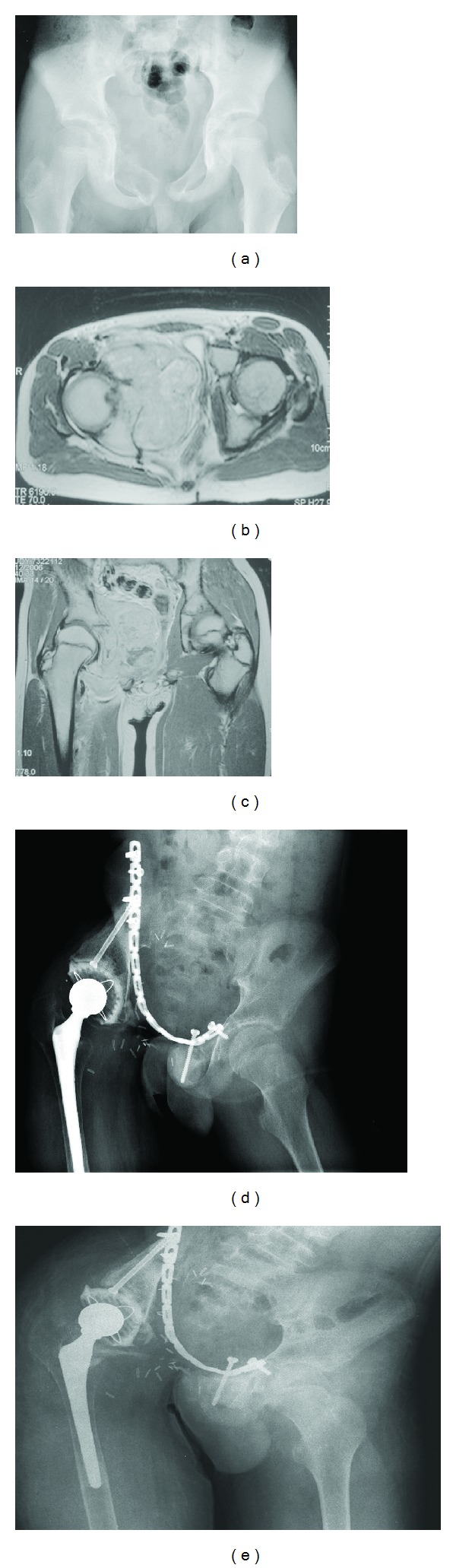
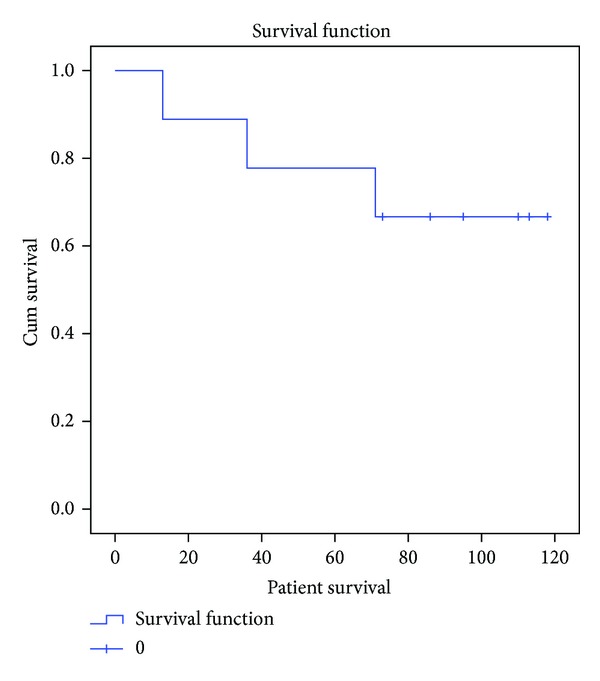
Reconstruction after the resection of a pelvic tumor is a challenging procedure in orthopedic oncology. The main advantage of allograft reconstruction is restoration of the bony architecture of the complex pelvic region. However, high complication rates such as infection and allograft resorption had been reported in the literature. In this study, we aimed to retrospectively review nine patients treated with pelvic resection and structural pelvic allograft reconstruction. Functional results, complications, and survival of the patients and the allografts were evaluated. At a mean follow-up of 79 months, three patients were dead. Major complications were detected in eight of the nine patients. Infection (four of the nine patients) and allograft resorption (three of the nine patients) were the most common causes of failure. The cumulative survival of the patients was 66.7 percent at 70 months. However, allograft survival was only 26.7 percent at 60 months. Mean MSTS score was 69. In conclusion, we suggest that other reconstruction options should be preferred after pelvic resections because of the high complication rates associated with massive allograft reconstruction.
Figures

References
-
- Carter SR, Eastwood DM, Grimer RJ, Sneath RS. Hindquarter amputation for tumours of the musculoskeletal system. Journal of Bone and Joint Surgery B. 1990;72(3):490–493. - PubMed
-
- Mankin HJ, Doppelt S, Tomford W. Clinical experience with allograft implantation. The first ten years. Clinical Orthopaedics and Related Research. 1983;174:69–86. - PubMed
-
- Aydinli U, Ozturk C, Yalcinkaya U, Tirelioglu O, Ersozlu S. Limb-sparing surgery for primary malignant tumours of the pelvis. Acta Orthopaedica Belgica. 2004;70(5):417–422. - PubMed
-
- Johnson JTH. Reconstruction of the pelvic ring following tumor resection. Journal of Bone and Joint Surgery A. 1978;60(6):747–751. - PubMed
-
- Aboulafia AJ, Buch R, Mathews J, Li W, Malawer MM. Reconstruction using the saddle prosthesis following excision of primary and metastatic periacetabular tumors. Clinical Orthopaedics and Related Research. 1995;(314):203–213. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
