

Altered islet function and insulin clearance cause hyperinsulinemia in gastric bypass patients with symptoms of postprandial hypoglycemia
- PMID: 24617664
- PMCID: PMC4037736
- DOI: 10.1210/jc.2013-2686
Altered islet function and insulin clearance cause hyperinsulinemia in gastric bypass patients with symptoms of postprandial hypoglycemia
Abstract
Context: Postprandial hypoglycemia, a late complication of gastric bypass (GB) surgery, is associated with an exaggerated insulin response to meal ingestion.
Objective: The purpose of this study was to characterize insulin secretion and other glucoregulatory hormone responses to meal ingestion after GB based on hypoglycemia and clinical symptoms.
Methods: We conducted a cross-sectional analysis of insulin secretion rate and islet and gastrointestinal hormone responses to liquid mixed meal ingestion in 65 subjects with GB and 11 body mass index-matched controls without surgery. The GB subjects were stratified by clinical history for analysis of their responses to the test meal.
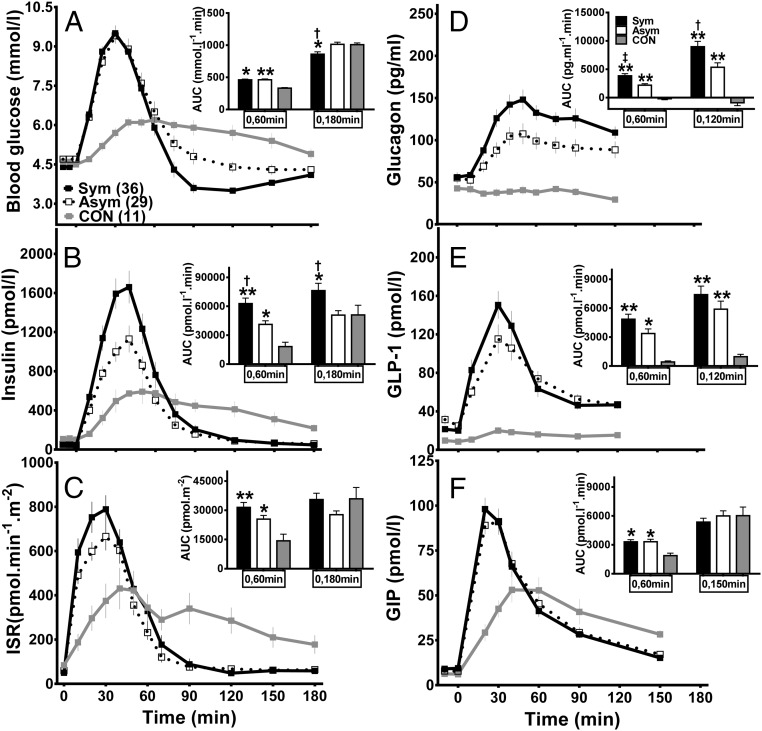
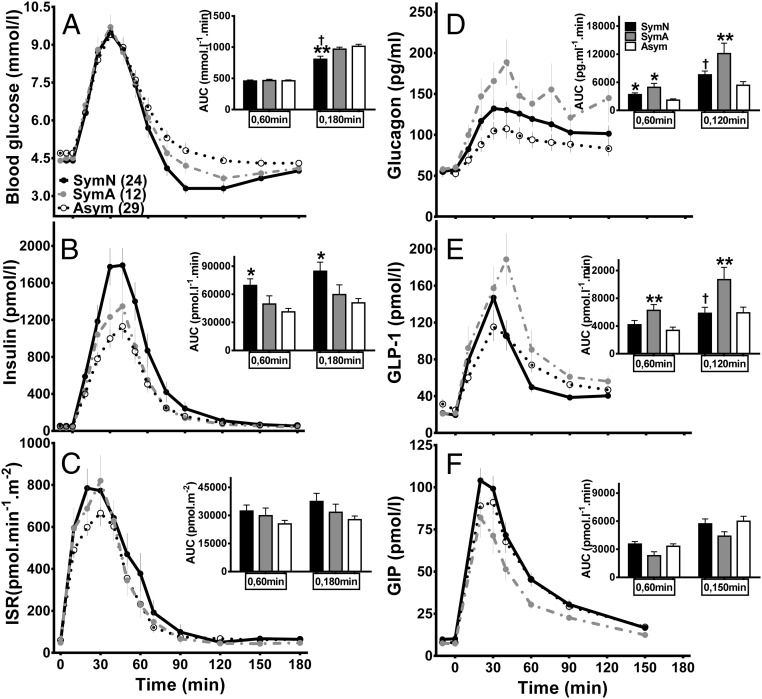
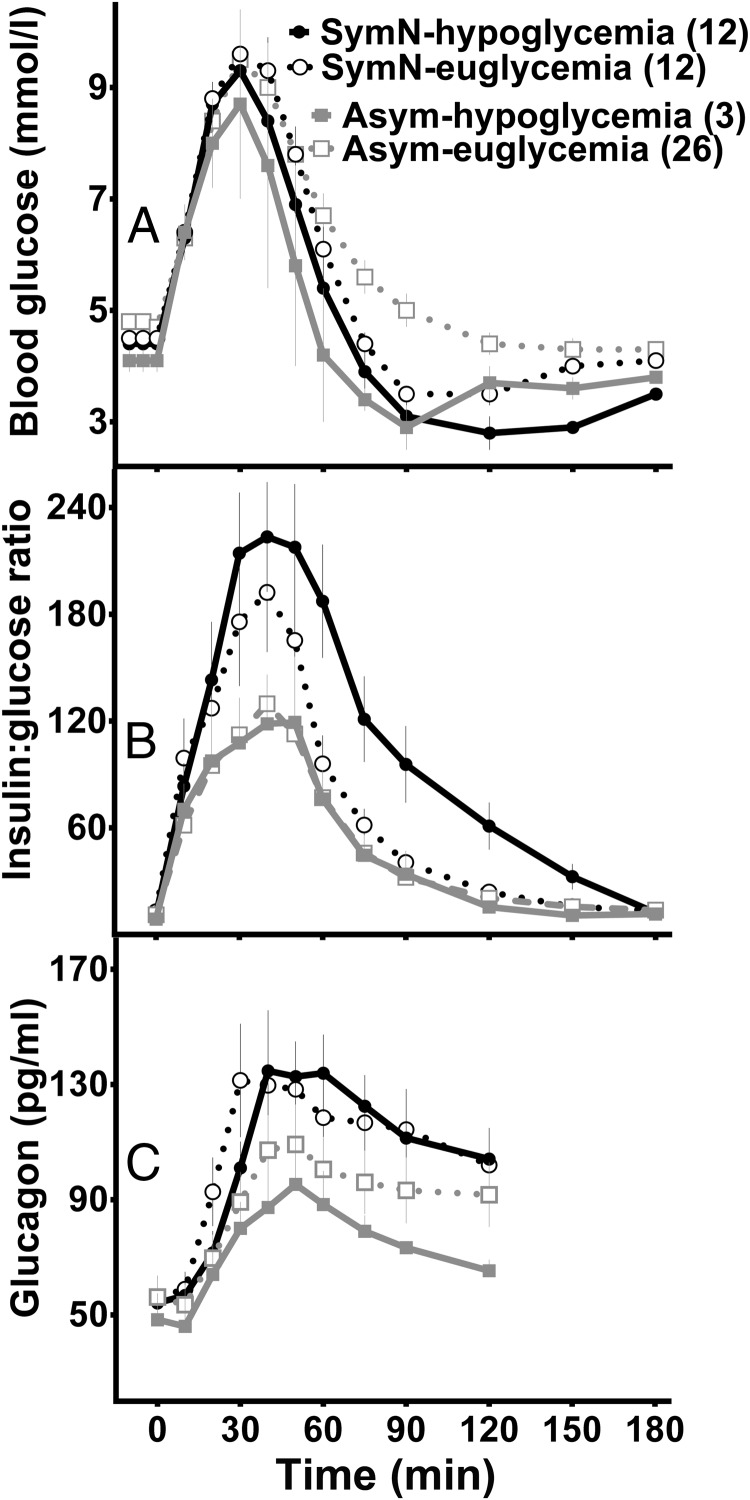
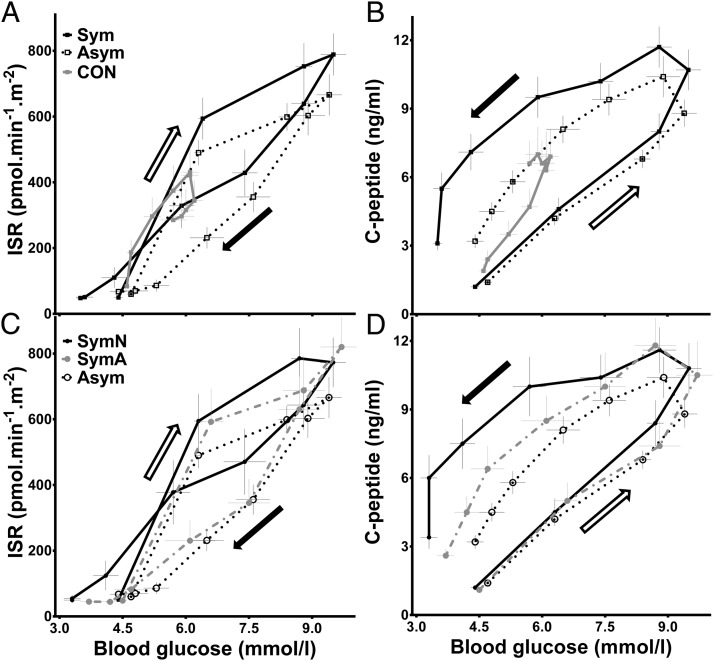
Results: The glucose and insulin responses to meal ingestion were shifted upward and to the left after GB, with the largest early insulin response and the lowest nadir glucose levels in patients with a history of hypoglycemia, particularly those with neuroglycopenic symptoms. Hypoglycemic GB subjects had lower postprandial insulin clearance rates and higher insulin secretion rates during the glucose decline after the test meal. Meal-induced glucagon was enhanced in all GB subjects but did not differ between subjects who did and did not develop hypoglycemia. Plasma gastric inhibitory polypeptide and glucagon-like peptide-1 concentrations did not differ between asymptomatic and neuroglycopenic GB subjects.
Conclusion: Among GB subjects with a clinical history of hypoglycemia, hyperinsulinemia is the result of inappropriate insulin secretion and reduced insulin clearance. In subjects with symptoms of postprandial hypoglycemia, insulin secretion is higher in the latter stages of meal glucose clearance, and despite elevated meal-induced glucagon, there is no further response to hypoglycemia. These abnormalities in islet function are most pronounced in subjects who report neuroglycopenic symptoms.
Figures
References
-
- Jørgensen NB, Jacobsen SH, Dirksen C, et al. Acute and long-term effects of Roux-en-Y gastric bypass on glucose metabolism in subjects with type 2 diabetes and normal glucose tolerance. Am J Physiol Endocrinol Metab. 2012;303:E122–E131 - PubMed
-
- Goldfine AB, Mun EC, Devine E, et al. Patients with neuroglycopenia after gastric bypass surgery have exaggerated incretin and insulin secretory responses to a mixed meal. J Clin Endocrinol Metab. 2007;92:4678–4685 - PubMed
-
- Roslin M, Damani T, Oren J, Andrews R, Yatco E, Shah P. Abnormal glucose tolerance testing following gastric bypass demonstrates reactive hypoglycemia. Surg Endosc. 2011;25:1926–1932 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
