

Myocardial T1 mapping: techniques and potential applications
- PMID: 24617686
- PMCID: PMC4358720
- DOI: 10.1148/rg.342125121
Myocardial T1 mapping: techniques and potential applications
Abstract
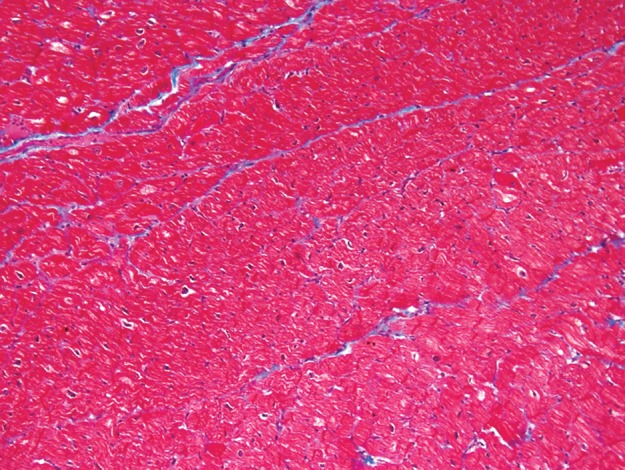
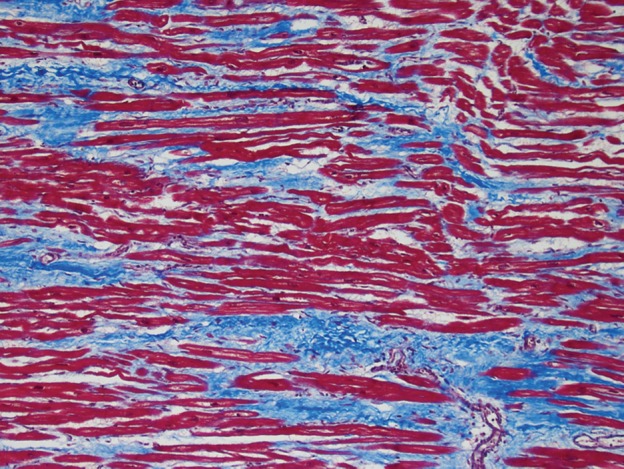
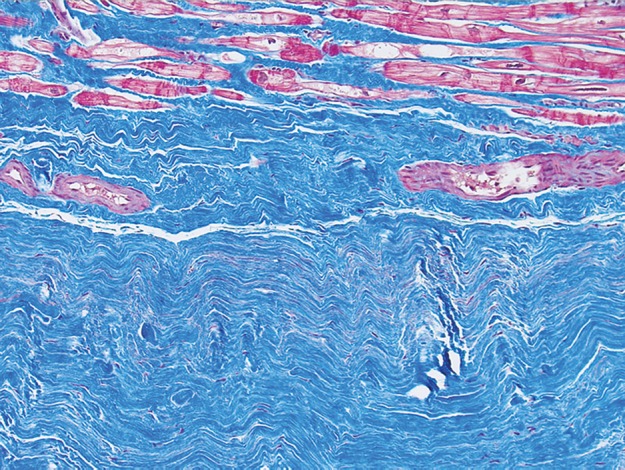
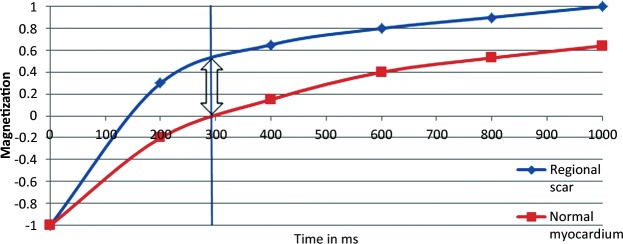
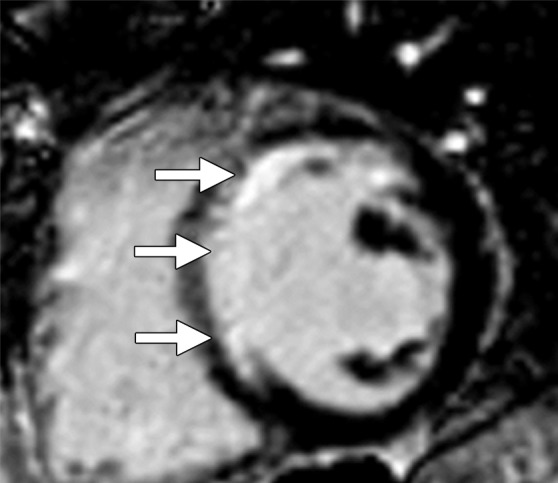
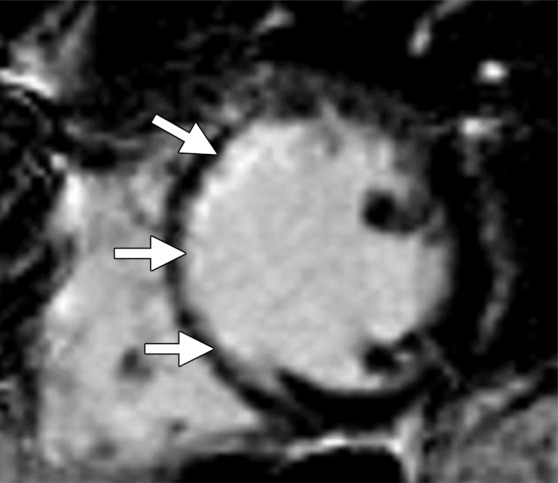
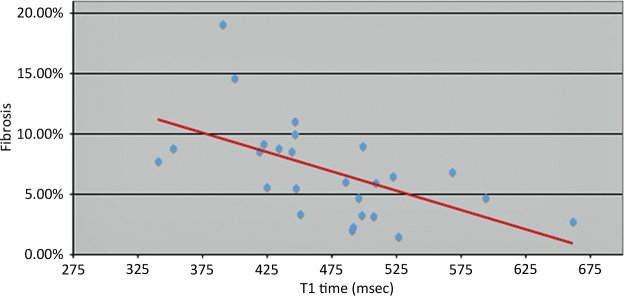
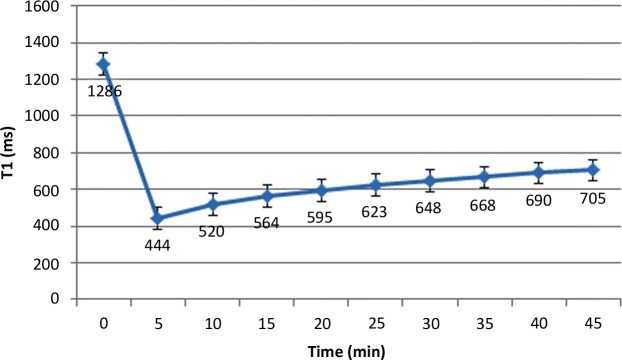
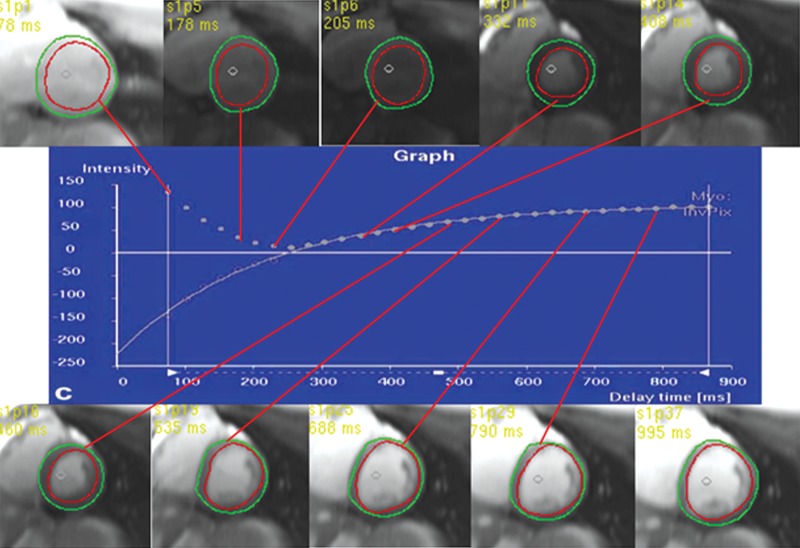
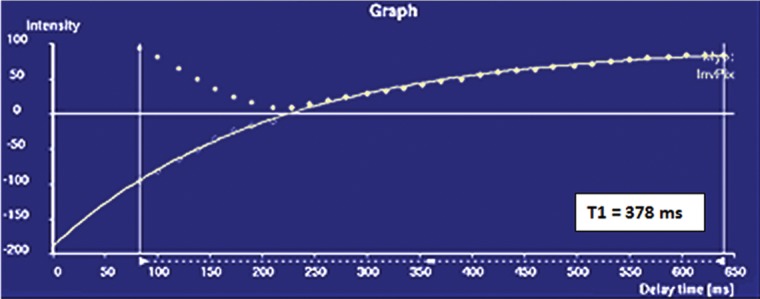
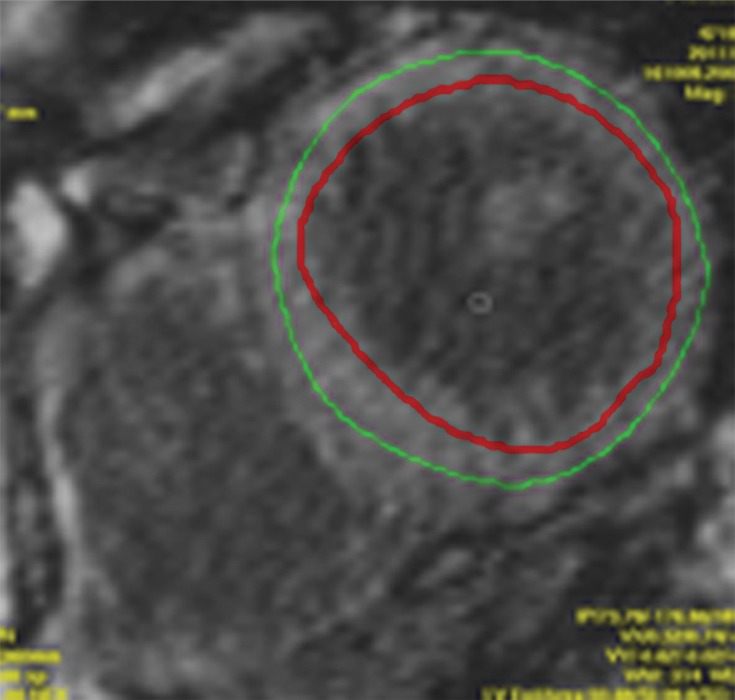
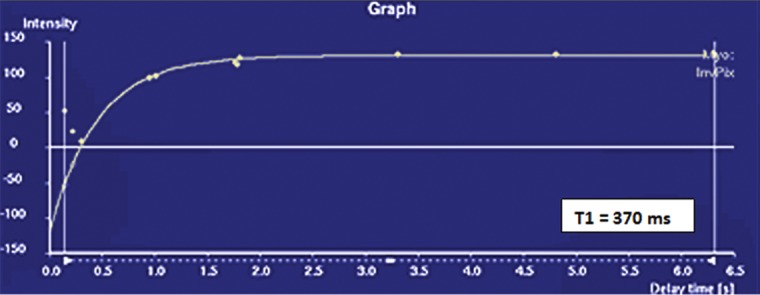
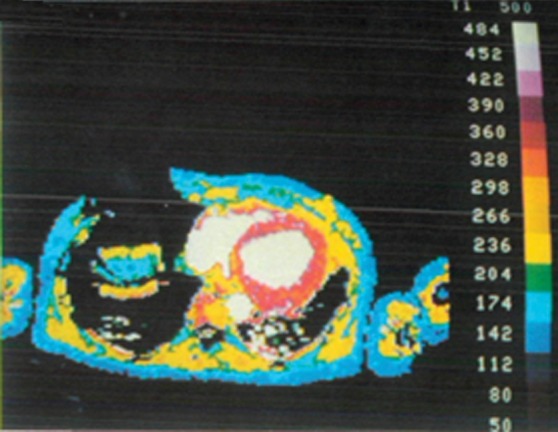
Myocardial fibrosis is a common endpoint in a variety of cardiac diseases and a major independent predictor of adverse cardiac outcomes. Short of histopathologic analysis, which is limited by sampling bias, most diagnostic modalities are limited in their depiction of myocardial fibrosis. Cardiac magnetic resonance (MR) imaging has the advantage of providing detailed soft-tissue characterization, and a variety of novel quantification methods have further improved its usefulness. Contrast material-enhanced cardiac MR imaging depends on differences in signal intensity between regions of scarring and adjacent normal myocardium. Diffuse myocardial fibrosis lacks these differences in signal intensity. Measurement of myocardial T1 times (T1 mapping) with gadolinium-enhanced inversion recovery-prepared sequences may depict diffuse myocardial fibrosis and has good correlation with ex vivo fibrosis content. T1 mapping calculates myocardial T1 relaxation times with image-based signal intensities and may be performed with standard cardiac MR imagers and radiologic workstations. Myocardium with diffuse fibrosis has greater retention of contrast material, resulting in T1 times that are shorter than those in normal myocardium. Early studies have suggested that diffuse myocardial fibrosis may be distinguished from normal myocardium with T1 mapping. Large multicenter studies are needed to define the role of T1 mapping in developing prognoses and therapeutic assessments. However, given its strengths as a noninvasive method for direct quantification of myocardial fibrosis, T1 mapping may eventually play an important role in the management of cardiac disease.
© RSNA, 2014.
Figures







References
-
- Kwong RY, Chan AK, Brown KA, et al. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation 2006;113(23):2733–2743. - PubMed
-
- Assomull RG, Prasad SK, Lyne J, et al. Cardiovascular magnetic resonance, fibrosis, and prognosis in dilated cardiomyopathy. J Am Coll Cardiol 2006;48(10):1977–1985. - PubMed
-
- Dweck MR, Joshi S, Murigu T, et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol 2011; 58(12):1271–1279. - PubMed
-
- Becker AE, Heijmans CD, Essed CE. Chronic non-ischaemic congestive heart disease and endomyocardial biopsies: worth the extra? Eur Heart J 1991; 12(2):218–223. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
