

Subcutaneous treprostinil is well tolerated with infrequent site changes and analgesics
- PMID: 24618545
- PMCID: PMC4070817
- DOI: 10.1086/674304
Subcutaneous treprostinil is well tolerated with infrequent site changes and analgesics
Abstract
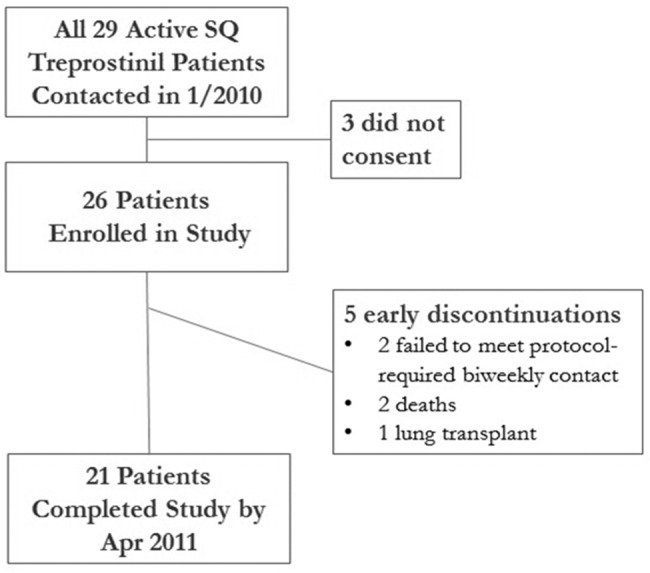
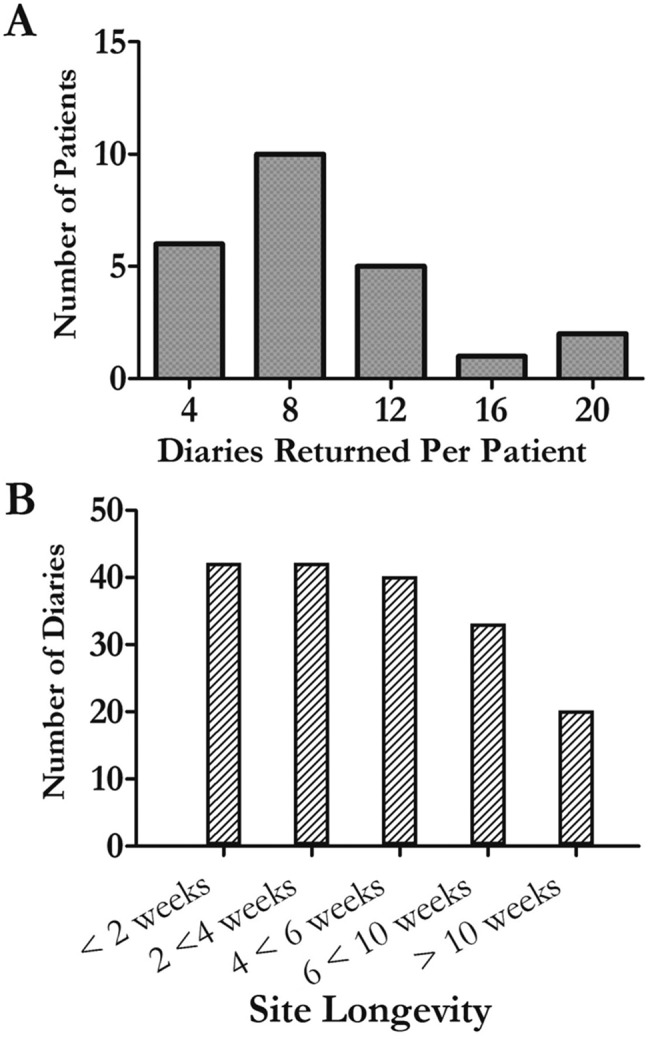
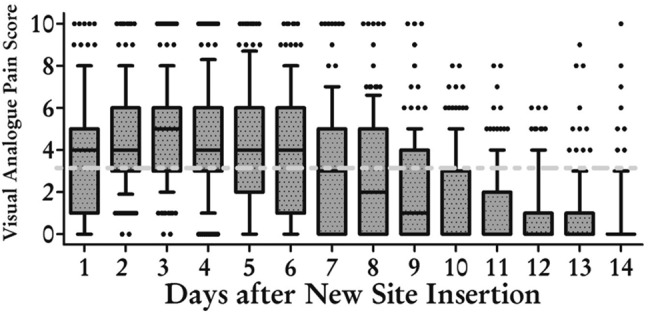
Abstract Continuous prostanoid infusions are recommended for patients with advanced pulmonary arterial hypertension. Infusion site pain has discouraged some physicians from considering subcutaneous (SQ) treprostinil therapy even though it has safety and convenience advantages over intravenous epoprostenol. We conducted a 1-year prospective study of patients utilizing SQ treprostinil. We provided counseling on infrequent site changes and a written analgesic protocol including narcotics. After placement of a new site, subjects recorded daily pain scores and analgesic use. Twenty-six of 29 patients consented, including 4 patients who had recently started therapy. They returned 203 diaries, and we captured every site change in a diary. Sixteen subjects returned 8 or fewer diaries during 12 months, and 20% of diaries documented only mild discomfort. The majority of diaries documented brief periods of severe pain, but this had generally abated by day 7. Contrary to published guidelines, infusion site pain was independent of treprostinil dose in a rigorous analysis. There were 3 significant local reactions but no systemic illness. No subject discontinued SQ treprostinil because of site discomfort. Subjects reported satisfaction with their treatment using a validated assessment, and quality-of-life scores were favorable. A strategy emphasizing infrequent site changes and early analgesia can facilitate use of SQ treprostinil. These data may allow physicians to consider treprostinil earlier in the treatment algorithm for this fatal disease.
Figures

 ,
,  for dose vs. total pain;
for dose vs. total pain;  ,
,  for maximum-intensity pain). B, A similar analysis for the volume of infusion and the pain was also negative. However, in the case of volume, there may have been a very loose relationship, and the statistical analyses left open this possibility (
for maximum-intensity pain). B, A similar analysis for the volume of infusion and the pain was also negative. However, in the case of volume, there may have been a very loose relationship, and the statistical analyses left open this possibility ( ,
,  for volume vs. total pain;
for volume vs. total pain;  ,
,  for maximum-intensity pain).
for maximum-intensity pain).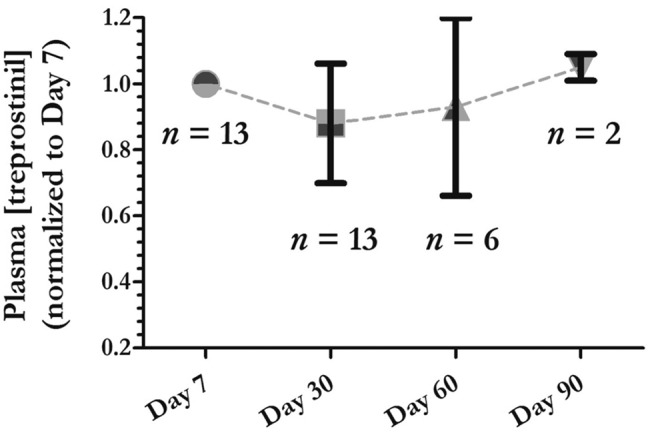
 at day 7,
at day 7,  at day 30,
at day 30,  at day 60,
at day 60,  at day 90. The raw data with actual treprostinil levels and doses (range, 47–170 ng/kg/min) are provided in Table 2.
at day 90. The raw data with actual treprostinil levels and doses (range, 47–170 ng/kg/min) are provided in Table 2.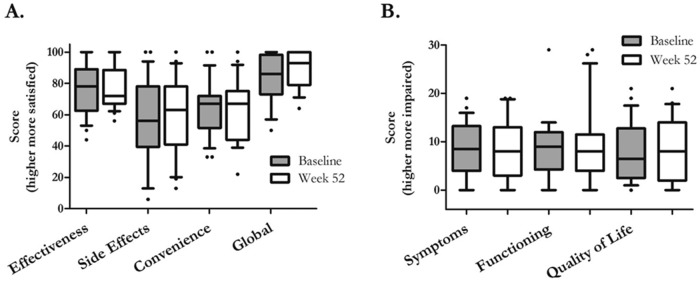
 at baseline;
at baseline;  at week 52.
at week 52.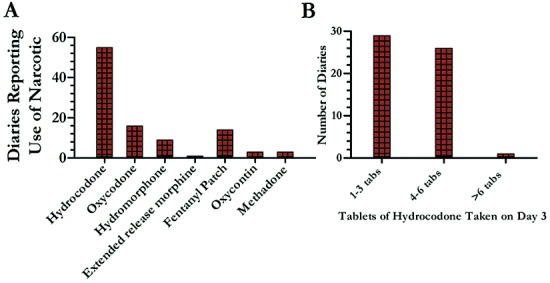
References
-
- Kawut SM, Horn EM, Berekashvili KK, et al. New predictors of outcome in idiopathic pulmonary arterial hypertension. Am J Cardiol 2005;95:199–203. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010;122:164–172. - PubMed
-
- Humbert M, Sitbon O, Yaici A, et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur Respir J 2010;36:549–555. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation 2010;122:156–163. - PubMed
-
- Rubin LJ, Mendoza J, Hood M, et al. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol): results of a randomized trial. Ann Int Med 1990;112:485–491. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
