

The effectiveness of financial incentives for health behaviour change: systematic review and meta-analysis
- PMID: 24618584
- PMCID: PMC3949711
- DOI: 10.1371/journal.pone.0090347
The effectiveness of financial incentives for health behaviour change: systematic review and meta-analysis
Abstract
Background: Financial incentive interventions have been suggested as one method of promoting healthy behaviour change.
Objectives: To conduct a systematic review of the effectiveness of financial incentive interventions for encouraging healthy behaviour change; to explore whether effects vary according to the type of behaviour incentivised, post-intervention follow-up time, or incentive value.
Data sources: Searches were of relevant electronic databases, research registers, www.google.com, and the reference lists of previous reviews; and requests for information sent to relevant mailing lists.
Eligibility criteria: Controlled evaluations of the effectiveness of financial incentive interventions, compared to no intervention or usual care, to encourage healthy behaviour change, in non-clinical adult populations, living in high-income countries, were included.
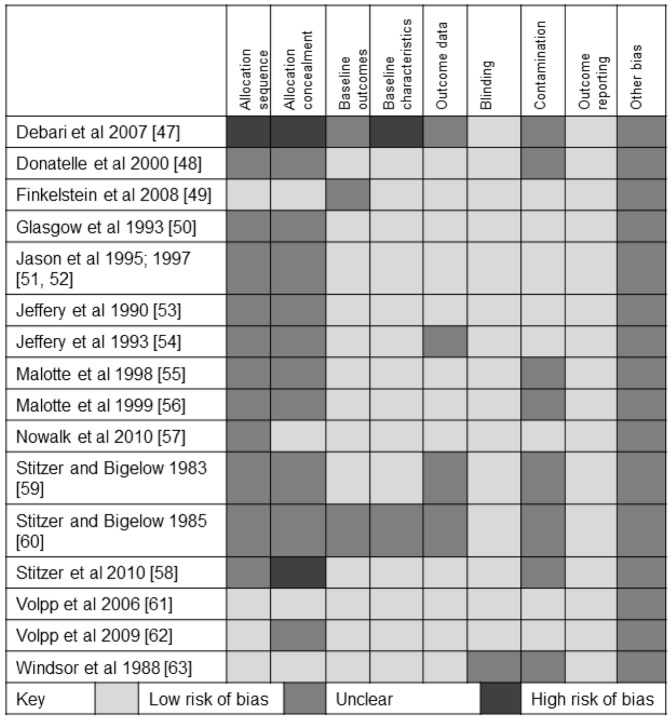
Study appraisal and synthesis: The Cochrane Risk of Bias tool was used to assess all included studies. Meta-analysis was used to explore the effect of financial incentive interventions within groups of similar behaviours and overall. Meta-regression was used to determine if effect varied according to post-intervention follow up time, or incentive value.
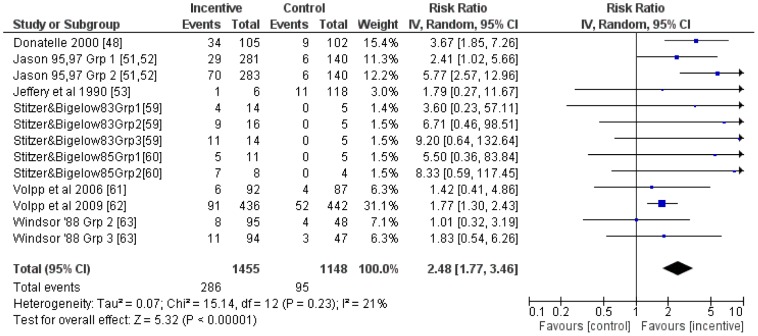
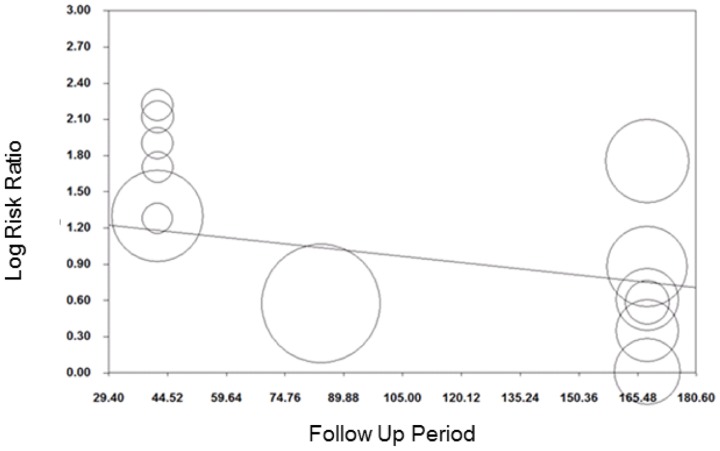
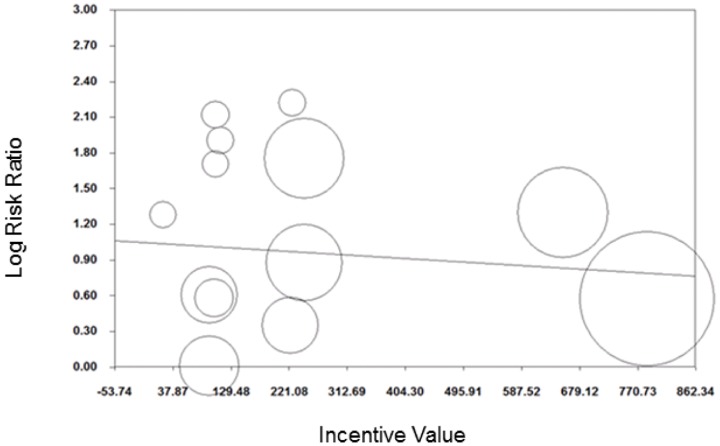
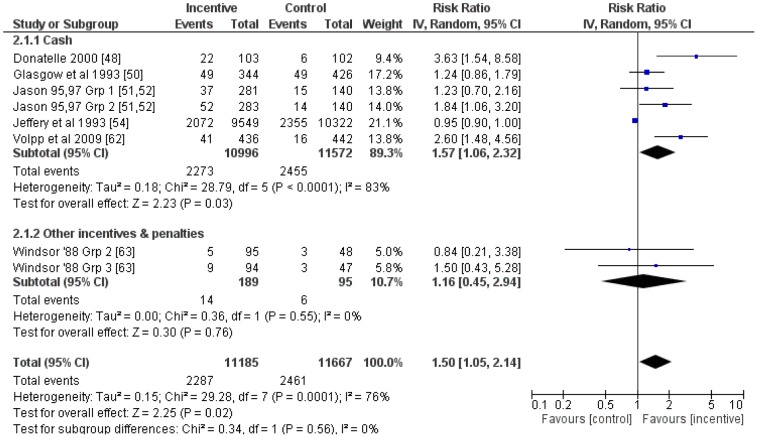
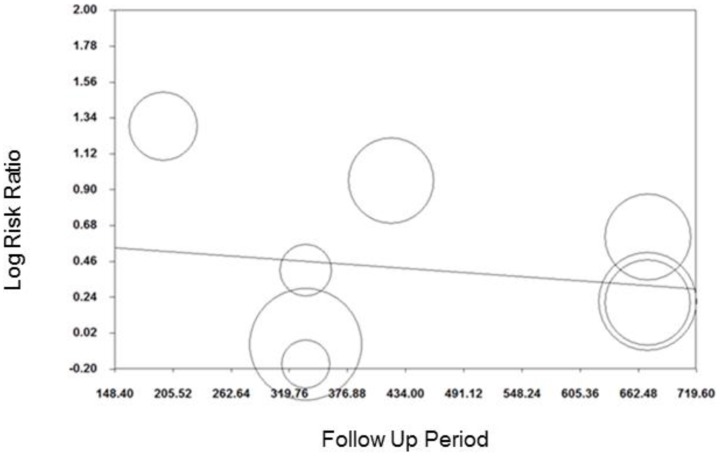
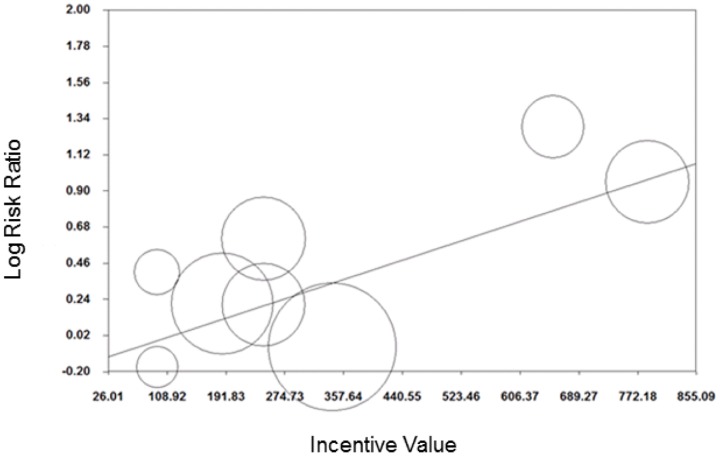
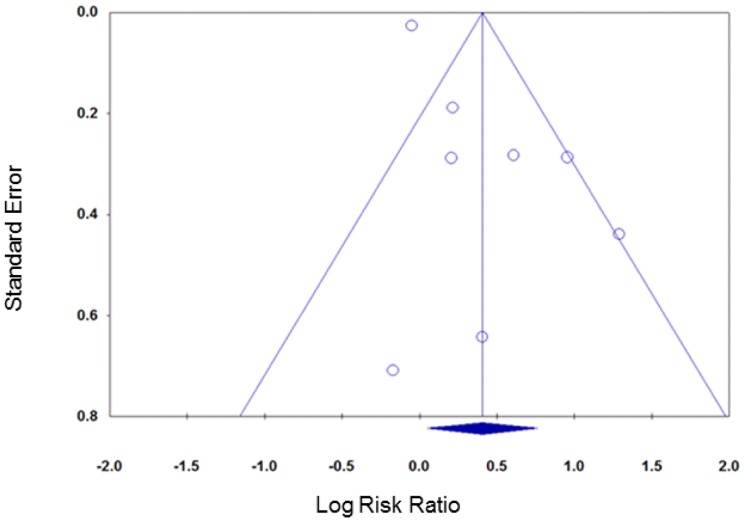
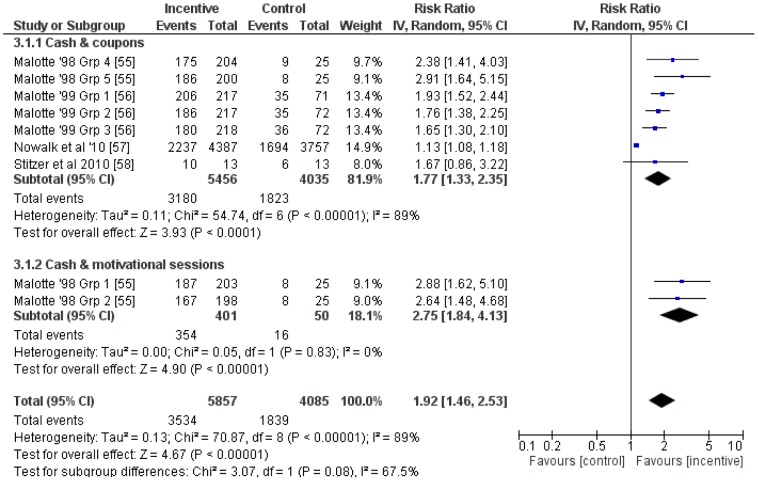
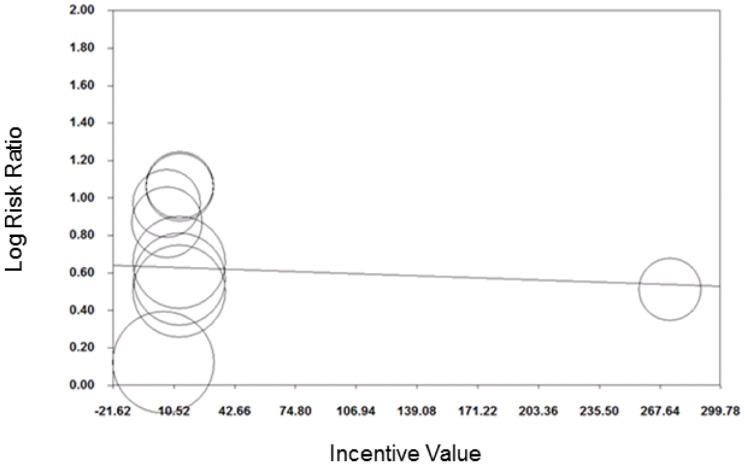
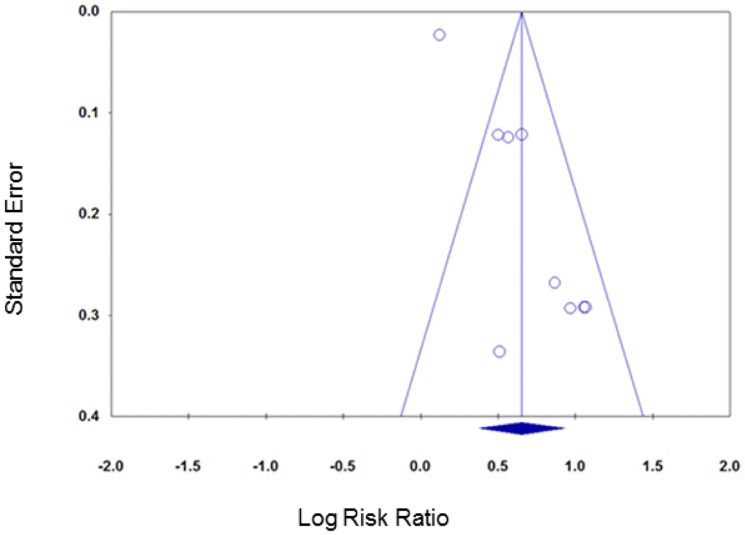
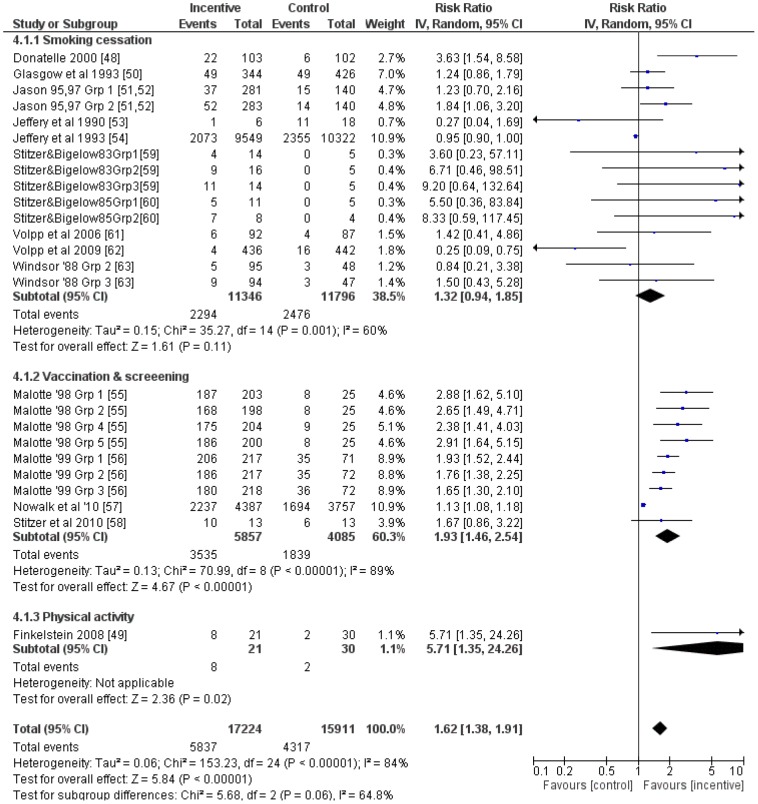
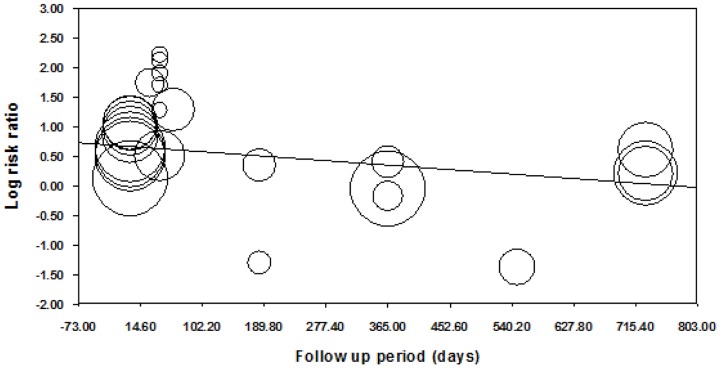
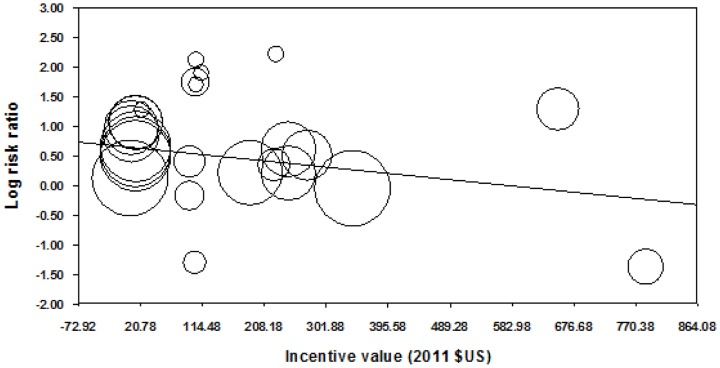
Results: Seventeen papers reporting on 16 studies on smoking cessation (n = 10), attendance for vaccination or screening (n = 5), and physical activity (n = 1) were included. In meta-analyses, the average effect of incentive interventions was greater than control for short-term (≤ six months) smoking cessation (relative risk (95% confidence intervals): 2.48 (1.77 to 3.46); long-term (>six months) smoking cessation (1.50 (1.05 to 2.14)); attendance for vaccination or screening (1.92 (1.46 to 2.53)); and for all behaviours combined (1.62 (1.38 to 1.91)). There was not convincing evidence that effects were different between different groups of behaviours. Meta-regression found some, limited, evidence that effect sizes decreased as post-intervention follow-up period and incentive value increased. However, the latter effect may be confounded by the former.
Conclusions: The available evidence suggests that financial incentive interventions are more effective than usual care or no intervention for encouraging healthy behaviour change.
Trial registration: PROSPERO CRD42012002393.
Conflict of interest statement
Figures


References
-
- Department of Health (1998) Our healthier nation: a contract for health. London: Her Majesty's Stationery Office.
-
- Department of Health (2004) Choosing health: making healthier choices easier. London: Her Majesty's Stationery Office.
-
- Eastwood P (2009) Health survey for England 2008: trend tables.
-
- Mazur JE (1987) An adjusting procedure for studying delayed reinforcement. In: Commons ML, Mazur JE, Nevin JA, Rachlin H, editors. Quantitative analysis of behaviour The effect of delay and intervening events on reinforcement value. Hillsdale, New Jersey: Erlbaum.
-
- Lowenstein G, Brennan T, Volpp K (2007) Asymmetric paternalism to improve health behaviors. Journal of the American Medical Association 298: 2415–2417. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
