

Trends in fluorescence image-guided surgery for gliomas
- PMID: 24618801
- PMCID: PMC4062574
- DOI: 10.1227/NEU.0000000000000344
Trends in fluorescence image-guided surgery for gliomas
Abstract
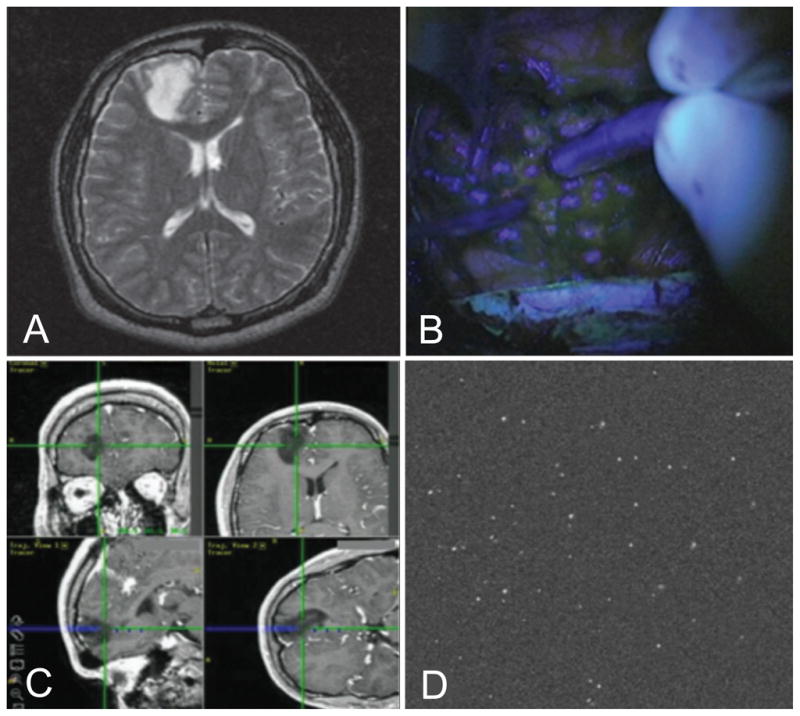
Mounting evidence suggests that a more extensive surgical resection is associated with an improved life expectancy for both low-grade and high-grade glioma patients. However, radiographically complete resections are not often achieved in many cases because of the lack of sensitivity and specificity of current neurosurgical guidance techniques at the margins of diffuse infiltrative gliomas. Intraoperative fluorescence imaging offers the potential to improve the extent of resection and to investigate the possible benefits of resecting beyond the radiographic margins. Here, we provide a review of wide-field and high-resolution fluorescence-imaging strategies that are being developed for neurosurgical guidance, with a focus on emerging imaging technologies and clinically viable contrast agents. The strengths and weaknesses of these approaches will be discussed, as well as issues that are being addressed to translate these technologies into the standard of care.
Conflict of interest statement
Figures



References
-
- Smith JS, Chang EF, Lamborn KR, et al. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J Clin Oncol. 2008;26:1338–1345. - PubMed
-
- Duffau H, Mandonnet E. The “onco-functional balance” in surgery for diffuse low-grade glioma: integrating the extent of resection with quality of life. Acta Neurochir (Wien ) 2013;155:951–957. - PubMed
-
- Duffau H. A new concept of diffuse (low-grade) glioma surgery. Adv Tech Stand Neurosurg. 2012;38:3–27. - PubMed
-
- Liao H, Noguchi M, Maruyama T, et al. An integrated diagnosis and therapeutic system using intra-operative 5-aminolevulinic-acid-induced fluorescence guided robotic laser ablation for precision neurosurgery. Med Image Anal. 2012;16:754–766. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
