

Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial
- PMID: 24618964
- PMCID: PMC4083455
- DOI: 10.1001/jama.2014.1719
Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial
Erratum in
-
Incorrect outcomes data.JAMA. 2015 Jun 9;313(22):2287. doi: 10.1001/jama.2015.4817. JAMA. 2015. PMID: 26057298 No abstract available.
Abstract
Importance: More than 300,000 surgeries are performed annually in the United States for pelvic organ prolapse. Sacrospinous ligament fixation (SSLF) and uterosacral ligament suspension (ULS) are commonly performed transvaginal surgeries to correct apical prolapse. Little is known about their comparative efficacy and safety, and it is unknown whether perioperative behavioral therapy with pelvic floor muscle training (BPMT) improves outcomes of prolapse surgery.
Objective: To compare outcomes between (1) SSLF and ULS and (2) perioperative BPMT and usual care in women undergoing surgery for vaginal prolapse and stress urinary incontinence.
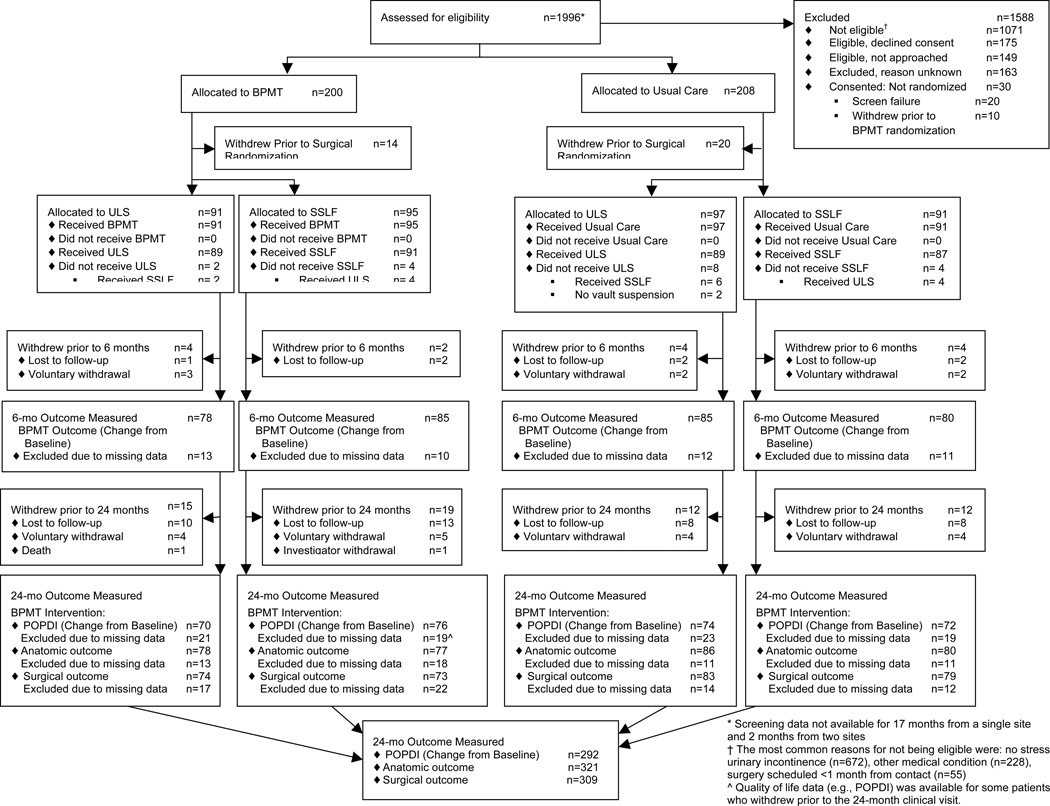
Design, setting, and participants: Multicenter, 2 × 2 factorial, randomized trial of 374 women undergoing surgery to treat both apical vaginal prolapse and stress urinary incontinence was conducted between 2008 and 2013 at 9 US medical centers. Two-year follow-up rate was 84.5%.
Interventions: The surgical intervention was transvaginal surgery including midurethral sling with randomization to SSLF (n = 186) or ULS (n = 188); the behavioral intervention was randomization to receive perioperative BPMT (n = 186) or usual care (n = 188).
Main outcomes and measures: The primary outcome for the surgical intervention (surgical success) was defined as (1) no apical descent greater than one-third into vaginal canal or anterior or posterior vaginal wall beyond the hymen (anatomic success), (2) no bothersome vaginal bulge symptoms, and (3) no re-treatment for prolapse at 2 years. For the behavioral intervention, primary outcome at 6 months was urinary symptom scores (Urinary Distress Inventory; range 0-300, higher scores worse), and primary outcomes at 2 years were prolapse symptom scores (Pelvic Organ Prolapse Distress Inventory; range 0-300, higher scores worse) and anatomic success.
Results: At 2 years, surgical group was not significantly associated with surgical success rates (ULS, 59.2% [93/157] vs SSLF, 60.5% [92/152]; unadjusted difference, -1.3%; 95% CI, -12.2% to 9.6%; adjusted odds ratio [OR], 0.9; 95% CI, 0.6 to 1.5) or serious adverse event rates (ULS, 16.5% [31/188] vs SSLF, 16.7% [31/186]; unadjusted difference, -0.2%; 95% CI, -7.7% to 7.4%; adjusted OR, 0.9; 95% CI, 0.5 to 1.6). Perioperative BPMT was not associated with greater improvements in urinary scores at 6 months (adjusted treatment difference, -6.7; 95% CI, -19.7 to 6.2), prolapse scores at 24 months (adjusted treatment difference, -8.0; 95% CI, -22.1 to 6.1), or anatomic success at 24 months.
Conclusions and relevance: Two years after vaginal surgery for prolapse and stress urinary incontinence, neither ULS nor SSLF was significantly superior to the other for anatomic, functional, or adverse event outcomes. Perioperative BPMT did not improve urinary symptoms at 6 months or prolapse outcomes at 2 years.
Trial registration: clinicaltrials.gov Identifier: NCT00597935.
Conflict of interest statement
The following authors report no such conflicts: Nygaard, Menefee, Norton, Weidner, Nguyen, Jakus-Waldman, Borello-France, Spino, Gantz, Warren, Wallace, Meikle
Figures
Comment in
-
Surgical techniques for apical vaginal prolapse.Am J Nurs. 2014 Sep;114(9):70. doi: 10.1097/01.NAJ.0000453763.00001.b8. Am J Nurs. 2014. PMID: 25166255 No abstract available.
-
Words of wisdom. Re: Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial.Eur Urol. 2015 Jan;67(1):172. doi: 10.1016/j.eururo.2014.09.044. Epub 2014 Nov 25. Eur Urol. 2015. PMID: 25528392 No abstract available.
-
Re: Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial.J Urol. 2015 Mar;193(3):943-4. doi: 10.1016/j.juro.2014.12.079. Epub 2014 Dec 18. J Urol. 2015. PMID: 25765407 No abstract available.
References
-
- FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Mesh Placement for Pelvic Organ Prolapse: US Food and Drug Administration. 2011 http://www.fda.gov/downloads/MedicalDevices/Safety/AlertsandNotices/UCM2....
-
- Brown JS, Waetjen LE, Subak LL, Thom DH, Van den Eeden S, Vittinghoff E. Pelvic organ prolapse surgery in the United States, 1997. Am J Obstet Gynecol. 2002;186(4):712–716. - PubMed
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–506. - PubMed
-
- Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979–1997. Am J Obstet Gynecol. 2003;188(1):108–115. - PubMed
-
- Shull BL. Pelvic organ prolapse: anterior, superior, and posterior vaginal segment defects. Am J Obstet Gynecol. 1999;181(1):6–11. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HD041261/HD/NICHD NIH HHS/United States
- U01 HD041249/HD/NICHD NIH HHS/United States
- U10 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054214/HD/NICHD NIH HHS/United States
- U01 HD069031/HD/NICHD NIH HHS/United States
- U10 HD041267/HD/NICHD NIH HHS/United States
- UG1 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054241/HD/NICHD NIH HHS/United States
- U10 HD041250/HD/NICHD NIH HHS/United States
- UG1 HD054214/HD/NICHD NIH HHS/United States
- U10 HD069006/HD/NICHD NIH HHS/United States
- UG1 HD041267/HD/NICHD NIH HHS/United States
- U10 HD054136/HD/NICHD NIH HHS/United States
- UG1 HD041261/HD/NICHD NIH HHS/United States
- UG1 HD054241/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
