

Microstructural impact of ischemia and bone marrow-derived cell therapy revealed with diffusion tensor magnetic resonance imaging tractography of the heart in vivo
- PMID: 24619466
- PMCID: PMC4034455
- DOI: 10.1161/CIRCULATIONAHA.113.005841
Microstructural impact of ischemia and bone marrow-derived cell therapy revealed with diffusion tensor magnetic resonance imaging tractography of the heart in vivo
Abstract
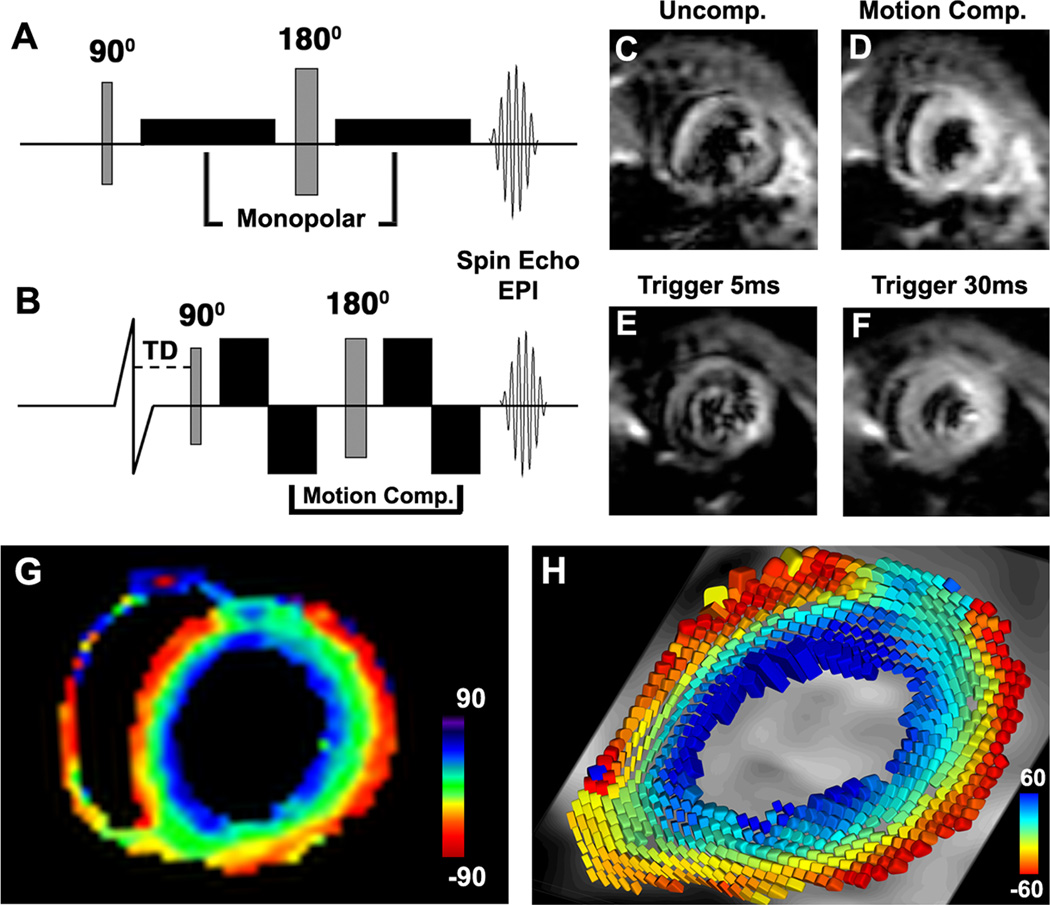
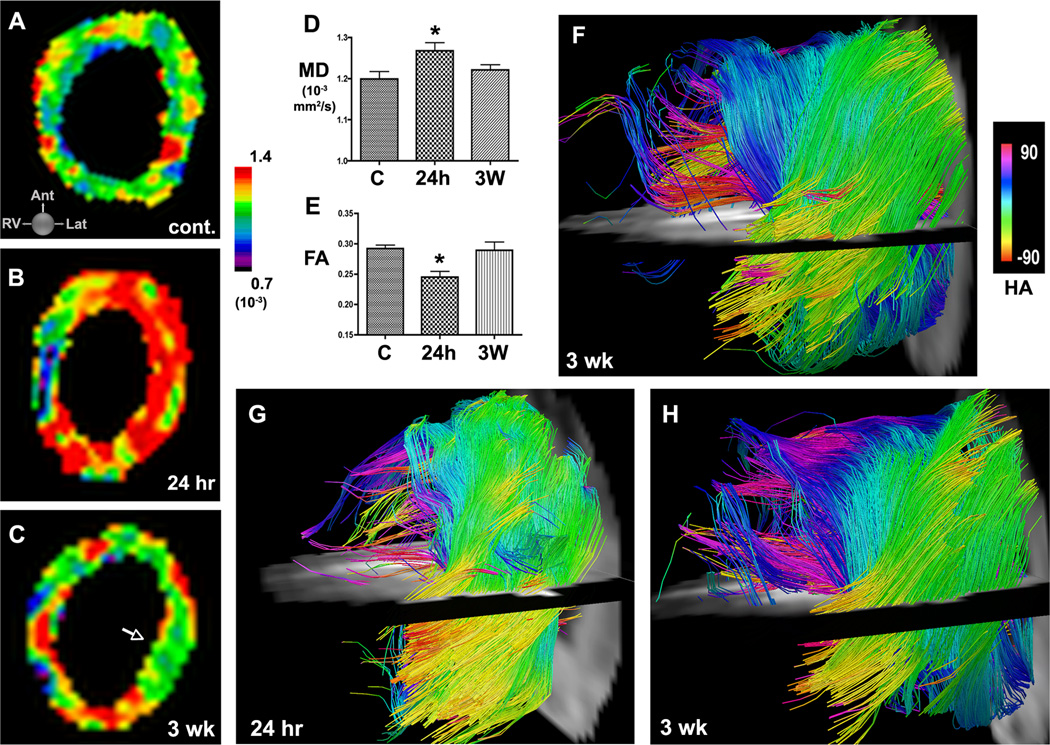
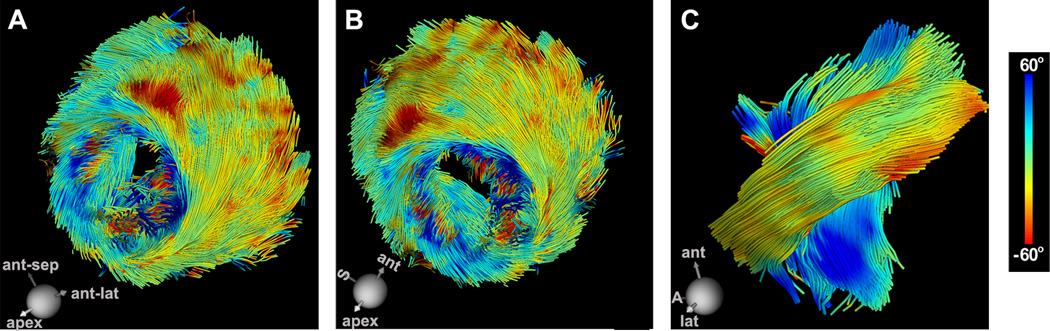
Background: The arrangement of myofibers in the heart is highly complex and must be replicated by injected cells to produce functional myocardium. A novel approach to characterize the microstructural response of the myocardium to ischemia and cell therapy, with the use of serial diffusion tensor magnetic resonance imaging tractography of the heart in vivo, is presented.
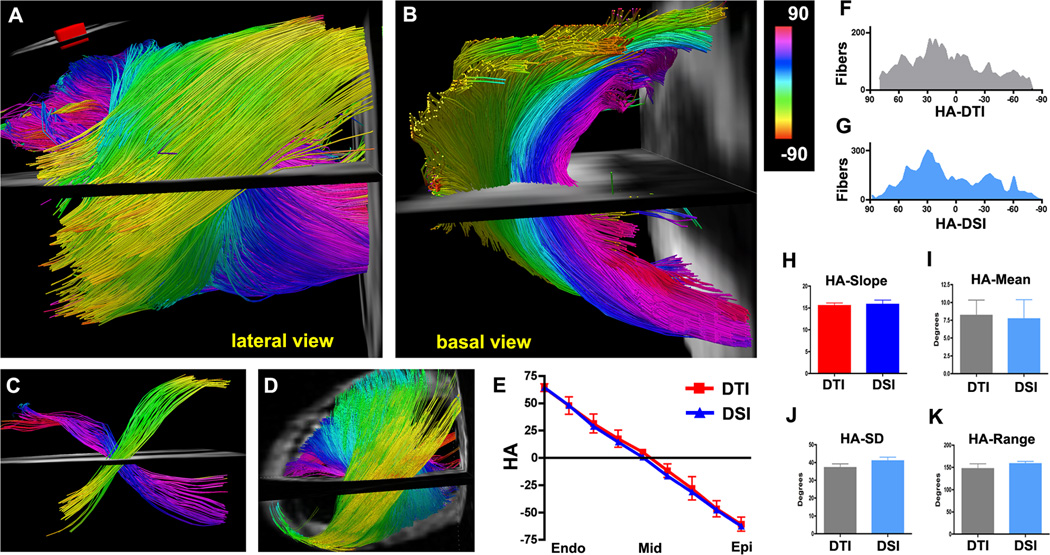
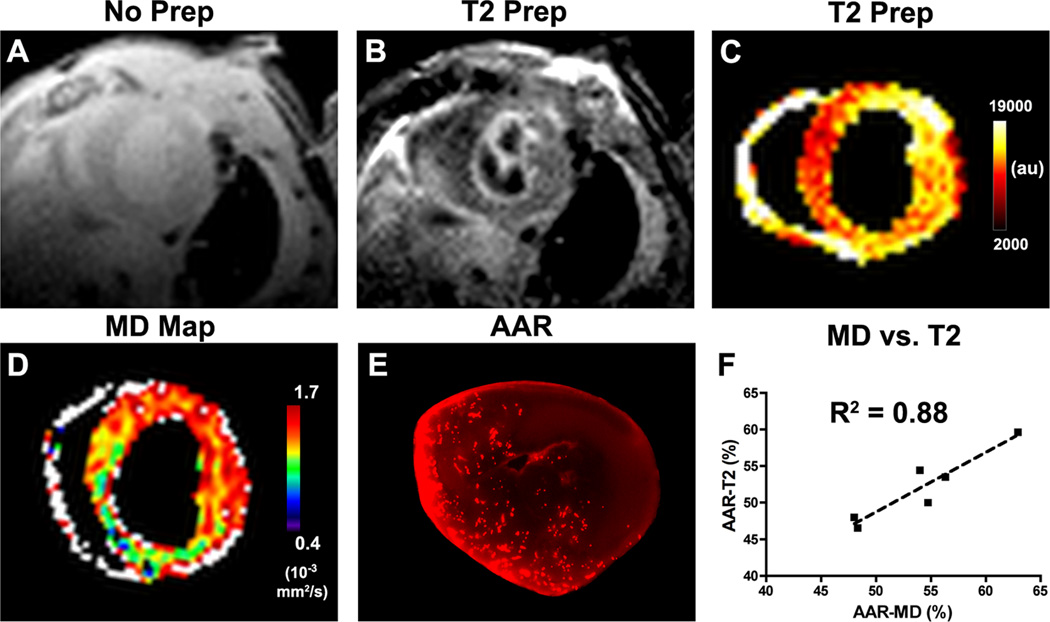
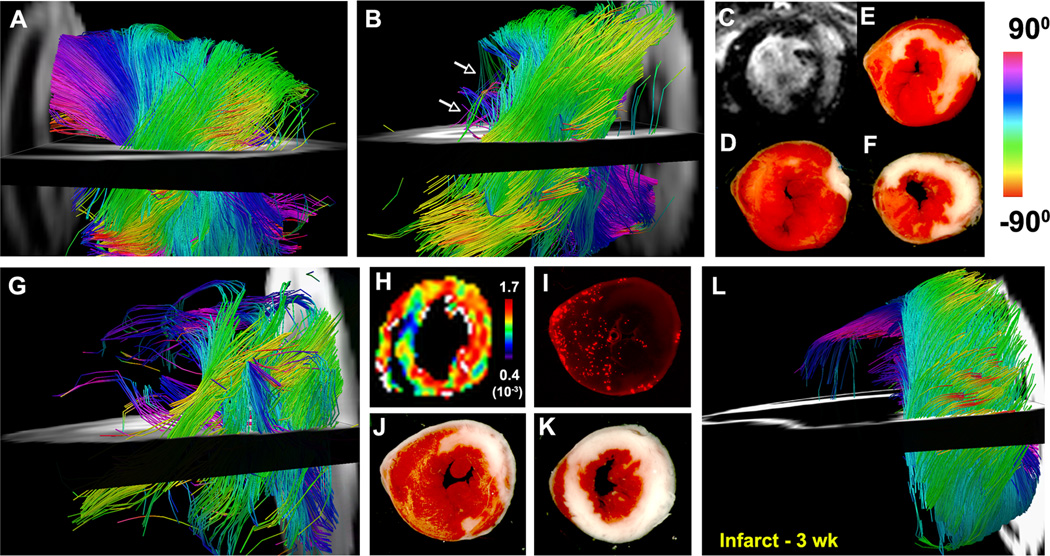
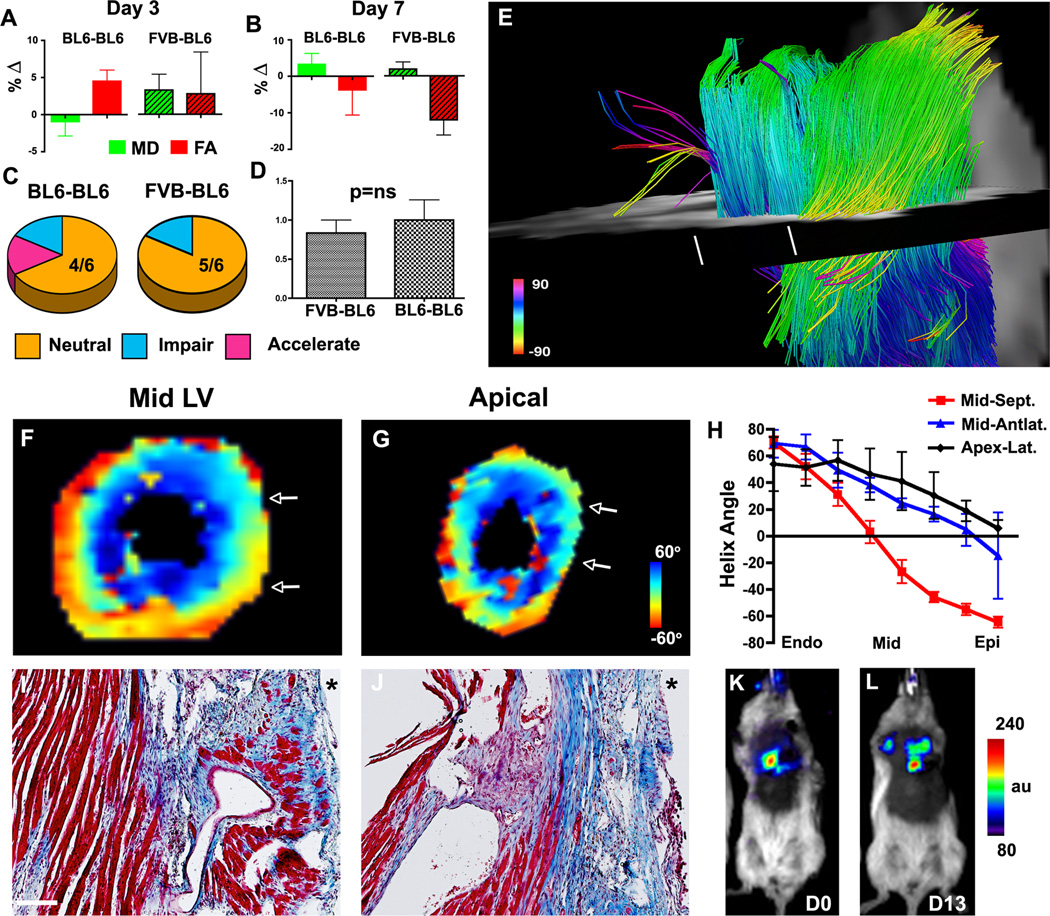
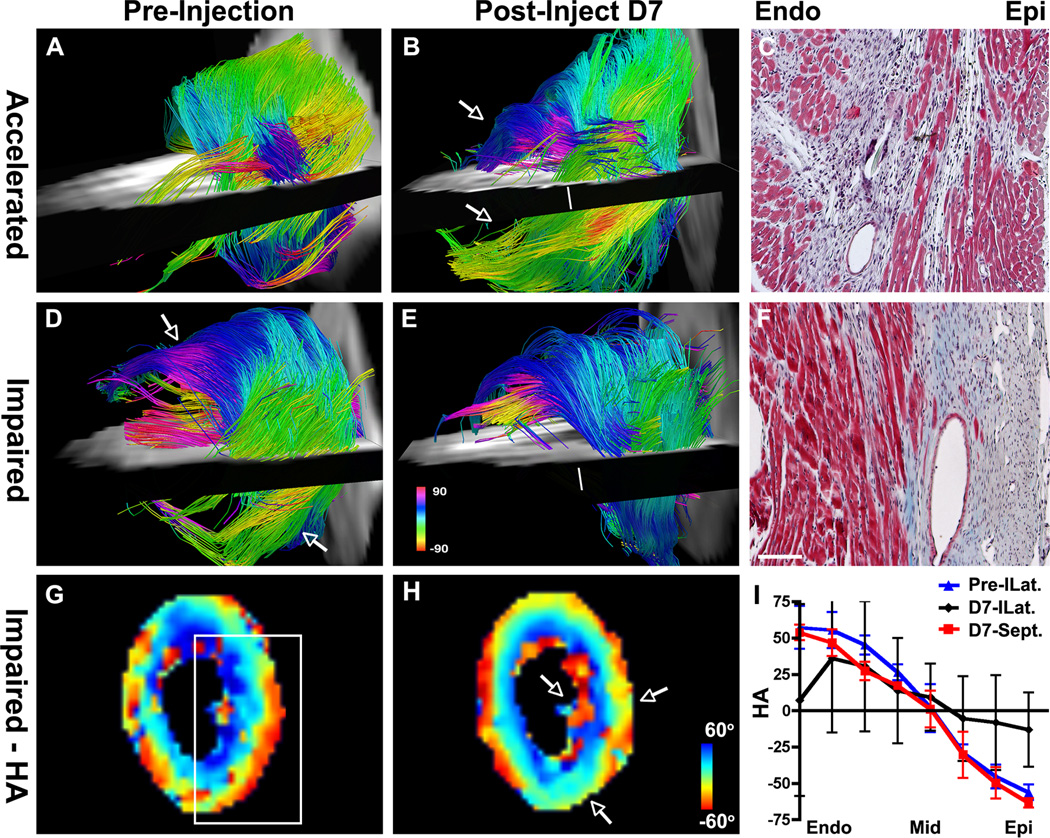
Methods and results: Validation of the approach was performed in normal (n=6) and infarcted mice (n=6) as well as healthy human volunteers. Mice (n=12) were then injected with bone marrow mononuclear cells 3 weeks after coronary ligation. In half of the mice the donor and recipient strains were identical, and in half the strains were different. A positive response to cell injection was defined by a decrease in mean diffusivity, an increase in fractional anisotropy, and the appearance of new myofiber tracts with the correct orientation. A positive response to bone marrow mononuclear cell injection was seen in 1 mouse. The response of the majority of mice to bone marrow mononuclear cell injection was neutral (9/12) or negative (2/12). The in vivo tractography findings were confirmed with histology.
Conclusions: Diffusion tensor magnetic resonance imaging tractography was able to directly resolve the ability of injected cells to generate new myofiber tracts and provided a fundamental readout of their regenerative capacity. A highly novel and translatable approach to assess the efficacy of cell therapy in the heart is thus presented.
Keywords: diffusion tensor imaging; diffusion tractography; ischemia; magnetic resonance imaging; myocardium; stem cell transplantation.
Figures
Comment in
-
Assessment of heart microstructure: from mouse to man.Circulation. 2014 Apr 29;129(17):1720-2. doi: 10.1161/CIRCULATIONAHA.114.009221. Epub 2014 Mar 11. Circulation. 2014. PMID: 24619467 Free PMC article. No abstract available.
References
-
- Rosenzweig A. Medicine. Cardiac regeneration. Science. 2012;338:1549–1550. - PubMed
-
- Streeter DD, Jr, Spotnitz HM, Patel DP, Ross J, Jr, Sonnenblick EH. Fiber orientation in the canine left ventricle during diastole and systole. Circ Res. 1969;24:339–347. - PubMed
-
- Scollan DF, Holmes A, Winslow R, Forder J. Histological validation of myocardial microstructure obtained from diffusion tensor magnetic resonance imaging. Am J Physiol. 1998;275:H2308–H2318. - PubMed
-
- Chen J, Song SK, Liu W, McLean M, Allen JS, Tan J, Wickline SA, Yu X. Remodeling of cardiac fiber structure after infarction in rats quantified with diffusion tensor MRI. Am J Physiol Heart Circ Physiol. 2003;285:H946–H954. - PubMed
-
- Wu EX, Wu Y, Nicholls JM, Wang J, Liao S, Zhu S, Lau CP, Tse HF. MR diffusion tensor imaging study of postinfarct myocardium structural remodeling in a porcine model. Magn Reson Med. 2007;58:687–695. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
