

Incidence and risk of sorafenib-induced hypertension: a systematic review and meta-analysis
- PMID: 24621095
- PMCID: PMC8031967
- DOI: 10.1111/jch.12273
Incidence and risk of sorafenib-induced hypertension: a systematic review and meta-analysis
Abstract
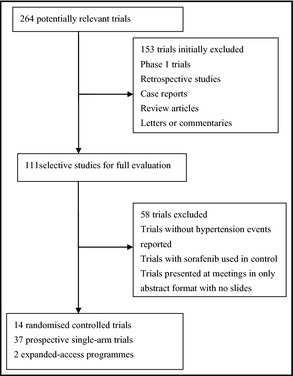
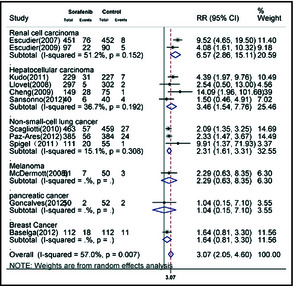
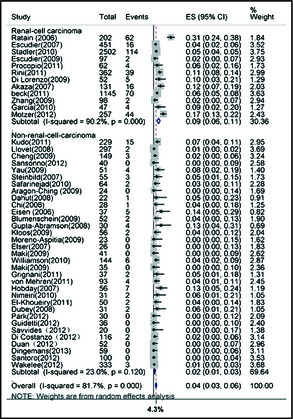
Hypertension is one of the major side effects of sorafenib, and reported incidences vary substantially among clinical trials. A systematic review was conducted using Medline, PubMed, Embase, and the Cochrane Library for all longitudinal studies to investigate the incidence and risk of hypertension events in cancer patients treated with sorafenib. A total of 14 randomized controlled trials and 39 prospective single-arm trials involving 13,555 patients were selected for the meta-analysis. The relative risk of all-grade and high-grade hypertension associated with sorafenib were 3.07 (95% confidence interval [CI], 2.05–4.60; P<.01) and 3.31 (95% CI, 2.21–4.95; P<.01), respectively. The overall incidence of sorafenib-induced all-grade and high-grade hypertension were 19.1% (95% CI, 15.8%–22.4%) and 4.3% (95% CI, 3.0%–5.5%), respectively. A significantly higher incidence of hypertension was noted in patients with renal cell carcinoma (RCC) compared with those with non-RCC malignancies (all-grade: 24.9% [95% CI, 19.7%–30.1%] vs 15.7%[95% CI, 12.1%–19.3%]; P<.05; high-grade:8.6% [95% CI, 6.0%–11.2%] vs 1.8% [95% CI, 0.9%–2.6%]; P<.05). The trials with median progression-free survival (PFS) longer than 5.3 months (mean PFS) demonstrated a significantly higher incidence of high-grade hypertension than trials with shorter PFS (6.3% [95% CI, 4.1%–8.5%] vs 2.6% [95% CI, 1.4%– 3.8%]; P<.05). Findings of the meta-analysis indicated a significantly high risk of sorafenib-induced hypertension. Patients with RCC have a significantly higher incidence of hypertension and the occurrence of hypertension may be associated with improved prognosis.
(c) 2014 Wiley Periodicals, Inc.
Figures

Comment in
-
VEGF pathway inhibitors-induced hypertension: next step in therapy.J Clin Hypertens (Greenwich). 2014 Aug;16(8):617. doi: 10.1111/jch.12348. Epub 2014 May 30. J Clin Hypertens (Greenwich). 2014. PMID: 24890259 Free PMC article. No abstract available.
References
-
- Wilhelm SM, Carter C, Tang L, et al. BAY 43‐9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64:7099–7109. - PubMed
-
- Verslype C, Rosmorduc O, Rougier P. Hepatocellular carcinoma: ESMO‐ESDO Clinical Practice Guidelines for diagnosis, treatment and follow‐up. Ann Oncol. 2012;23 (Suppl 7):vii41–vii48. - PubMed
-
- Escudier B, Eisen T, Porta C, et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow‐up. Ann Oncol. 2012;23 (Suppl 7):vii65–vii71. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
