

The STICH trial (Surgical Treatment for Ischemic Heart Failure): mode-of-death results
- PMID: 24621972
- PMCID: PMC3829618
- DOI: 10.1016/j.jchf.2013.04.012
The STICH trial (Surgical Treatment for Ischemic Heart Failure): mode-of-death results
Abstract
Objectives: This study sought to assess the effect of the addition of coronary artery bypass grafting (CABG) to medical therapy on mode of death in heart failure.
Background: Although CABG therapy is widely used in ischemic cardiomyopathy patients, there are no prospective clinical trial data on mode of death.
Methods: The STICH (Surgical Treatment for Ischemic Heart Failure ) trial compared the strategy of CABG plus medical therapy to medical therapy alone in 1,212 ischemic cardiomyopathy patients with reduced ejection fraction. A clinical events committee adjudicated deaths using pre-specified definitions for mode of death.
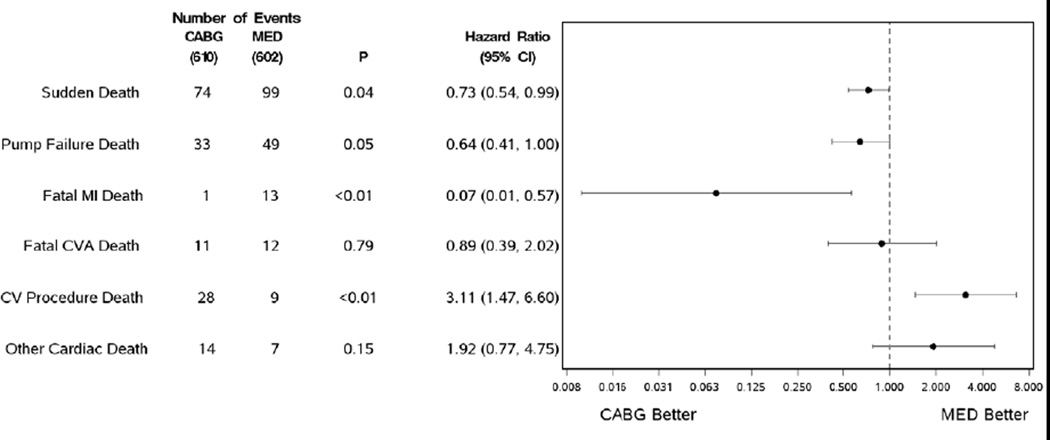
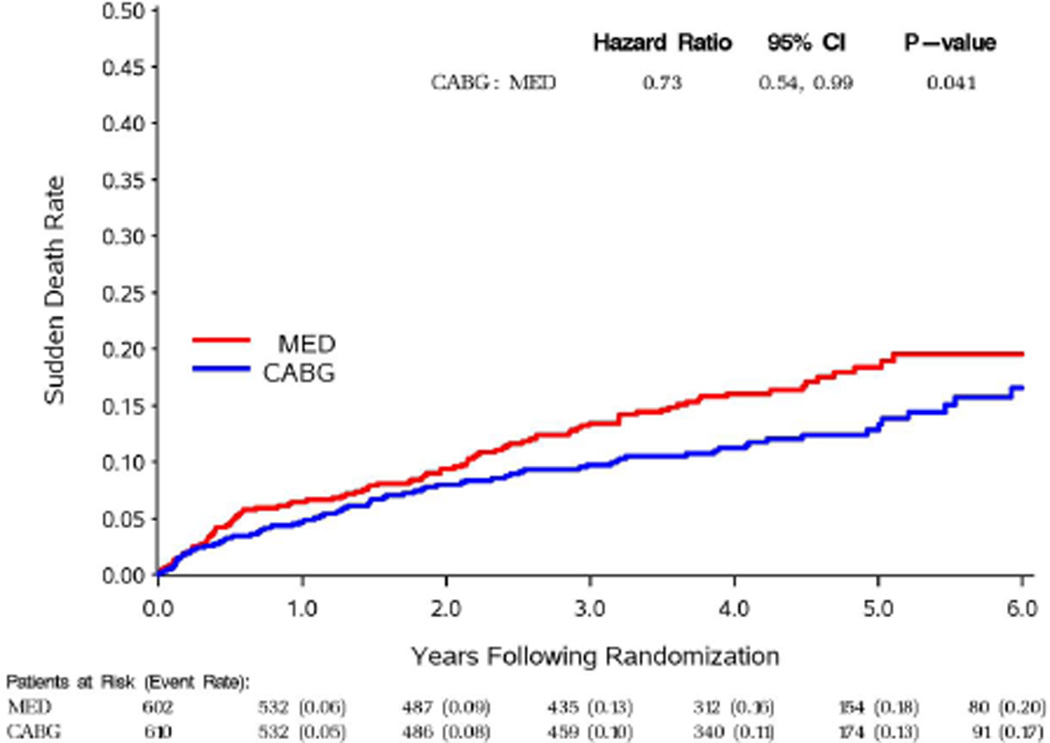
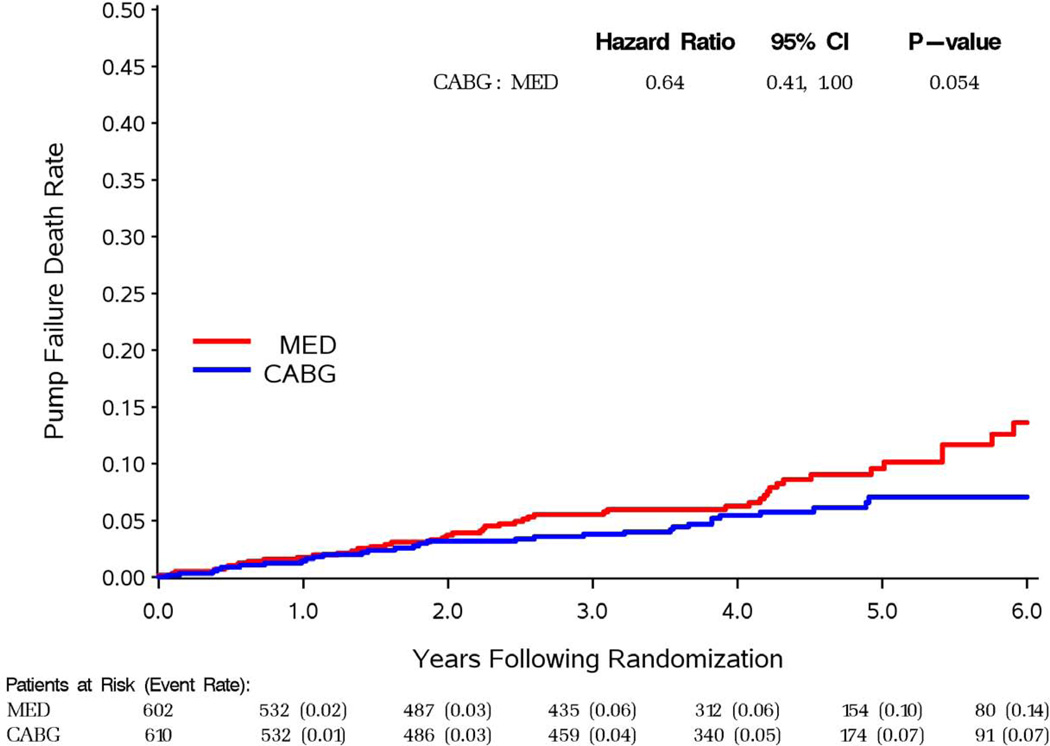
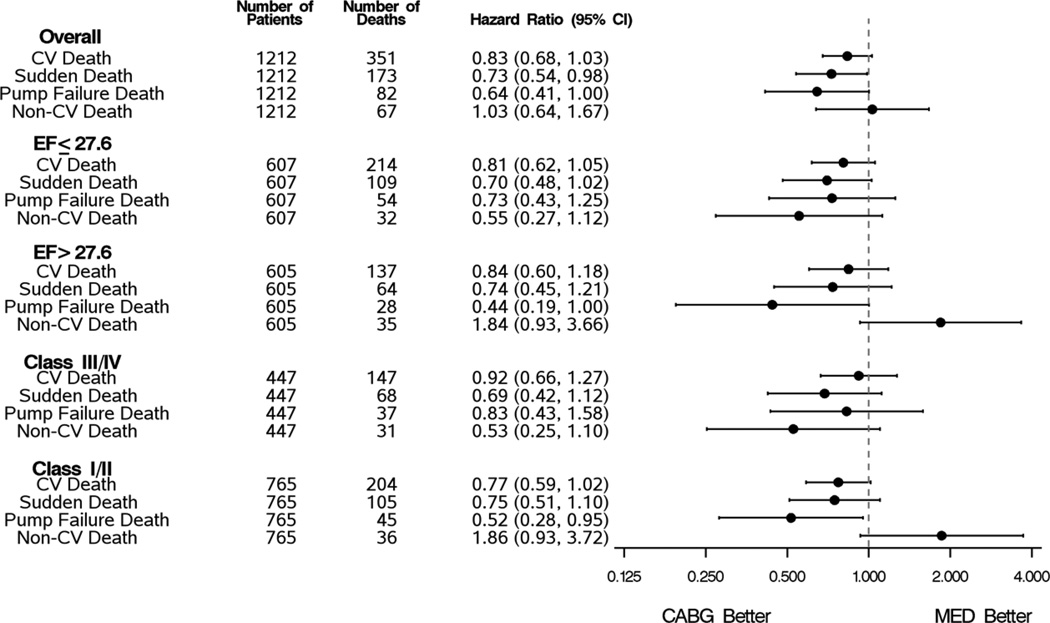
Results: In the STICH trial, there were 462 deaths over a median follow-up of 56 months. The addition of CABG therapy tended to reduce cardiovascular deaths (hazard ratio [HR]: 0.83; 95% confidence interval [CI]: 0.68 to 1.03; p = 0.09) and significantly reduced the most common modes of death: sudden death (HR: 0.73; 95% CI: 0.54 to 0.99; p = 0.041) and fatal pump failure events (HR: 0.64; 95% CI: 0.41 to 1.00; p = 0.05). Time-dependent estimates indicate that the protective effect of CABG principally occurred after 24 months in both categories. Deaths post-cardiovascular procedures were increased in CABG patients (HR: 3.11; 95% CI: 1.47 to 6.60), but fatal myocardial infarction deaths were lower (HR: 0.07; 95% CI: 0.01 to 0.57). Noncardiovascular deaths were infrequent and did not differ between groups.
Conclusions: In the STICH trial, the addition of CABG to medical therapy reduced the most common modes of death: sudden death and fatal pump failure events. The beneficial effects were principally seen after 2 years. Post-procedure deaths were increased in patients randomized to CABG, whereas myocardial infarction deaths were decreased.
Keywords: heart failure; mode of death; surgical.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348:2007–2018. - PubMed
-
- The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS) N Engl J Med. 1987;316:1429–1435. - PubMed
-
- The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325:293–302. - PubMed
-
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353:9–13. - PubMed
-
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) Lancet. 1999;353:2001–2007. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
