

Minimally invasive image-guided access for drainage of petrous apex lesions: a case report
- PMID: 24622019
- PMCID: PMC4001823
- DOI: 10.1097/MAO.0000000000000328
Minimally invasive image-guided access for drainage of petrous apex lesions: a case report
Abstract
Objective: In this case report, we present a novel, minimally invasive image-guided approach to drainage of a petrous apex lesion.
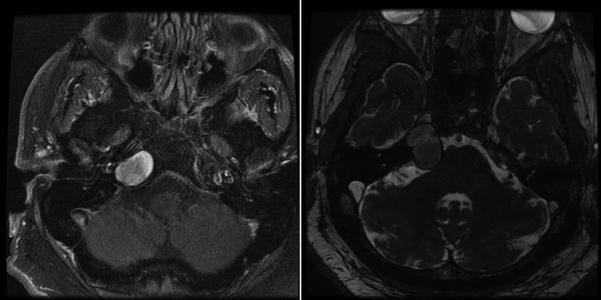
Patient(s): A 34-year-old man diagnosed with a petrous apex lesion consistent with cholesterol granuloma. The granuloma was large and caused mild compression of the brainstem with associated neurologic symptoms and seizure-like activity.
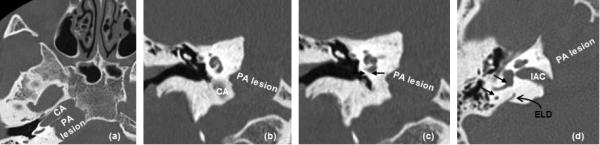
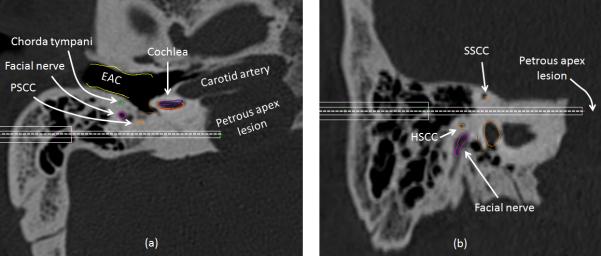
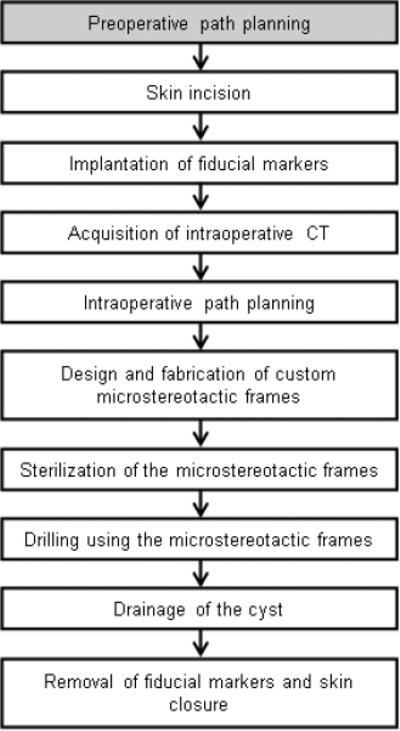
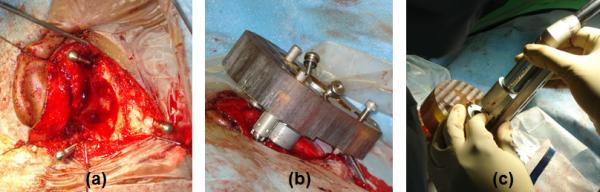
Interventions: Based on the anatomic location of the lesion, it was determined that the treatment plan would be to surgically drain the lesion via 2 linear paths-one after an infralabyrinthine approach and the other a subarcuate approach. Customized microstereotactic frames that mount on bone-implanted markers and constrain the drill along the desired path were used to accurately drill these desired paths and avoid damage to surrounding critical structures. After a simple mastoidectomy, the petrous apex was successfully reached without damage to vital adjacent structures by drilling the 2 linear channels using 2 custom microstereotactic frames.
Main outcome measures: Viscous brown liquid and debris was recovered by irrigating through one of the channels and suctioning through the other.
Results: Drainage of the petrous apex was successfully performed via 2 linear channels without any complications. Custom microstereotactic frames were used to accurately drill those linear channels. Postoperative CT ensured no complications. Postoperative course of the patient was remarkable with normal hearing and normal facial nerve function.
Conclusion: We presented a successful implementation of an image-guided approach to drain petrous apex.
Figures
Similar articles
-
[Excision and drainage of cholesterol granulomas of the petrous apex with preservation of hearing under computer-assisted navigation surgery (CANS)].Schweiz Med Wochenschr. 2000;Suppl 125:67S-70S. Schweiz Med Wochenschr. 2000. PMID: 11141944 German.
-
Drainage of a petrous apex cholesterol granuloma through an infracochlear approach.Am J Otolaryngol. 2020 Nov-Dec;41(6):102456. doi: 10.1016/j.amjoto.2020.102456. Epub 2020 Mar 13. Am J Otolaryngol. 2020. PMID: 32199711
-
[Infralabyrinthine approach for cholesterol granuloma of the petrous apex].Ann Otolaryngol Chir Cervicofac. 2000 Jun;117(3):174-82. Ann Otolaryngol Chir Cervicofac. 2000. PMID: 10863203 French.
-
Endoscopic Endonasal Transpterygoid Approach Using Pedicled Nasoseptal Flap for Petrous Apex Cholesterol Granuloma With Intraoperative Video.J Craniofac Surg. 2019 Sep;30(6):1833-1835. doi: 10.1097/SCS.0000000000005589. J Craniofac Surg. 2019. PMID: 31313683 Review.
-
Cholesterol granuloma in the petrous apex: case report and review.Acta Neurochir (Wien). 2001 Sep;143(9):947-52. doi: 10.1007/s007010170026. Acta Neurochir (Wien). 2001. PMID: 11685628 Review.
Cited by
-
Cholesterol Granulomas: A Comparative Meta-Analysis of Endonasal Endoscopic versus Open Approaches to the Petrous Apex.J Int Adv Otol. 2019 Aug;15(2):193-199. doi: 10.5152/iao.2019.5859. J Int Adv Otol. 2019. PMID: 31287439 Free PMC article.
-
Assessing the feasibility of the transmastoid infralabyrinthine approach without decompression of the jugular bulb to the extradural part of the petrous apex and petroclival junction prior to surgery.Acta Neurochir (Wien). 2024 Mar 26;166(1):151. doi: 10.1007/s00701-024-06044-8. Acta Neurochir (Wien). 2024. PMID: 38530445 Free PMC article.
-
Freehand Stereotactic Image-Guidance Tailored to Neurotologic Surgery.Front Surg. 2021 Oct 7;8:742112. doi: 10.3389/fsurg.2021.742112. eCollection 2021. Front Surg. 2021. PMID: 34692764 Free PMC article.
-
Decompression of the Jugular Bulb for Enhanced Infralabyrinthine Access to the Petroclival Region: A Quantitative Analysis.J Neurol Surg B Skull Base. 2016 Jun;77(3):249-59. doi: 10.1055/s-0035-1566302. Epub 2015 Nov 16. J Neurol Surg B Skull Base. 2016. PMID: 27175321 Free PMC article.
References
-
- Gore MR, Zanation AM, Ebert CS, Senior BA. Cholesterol granuloma of the petrous apex. Otolaryngol Clin North Am. 2011;44(5):1043–58. - PubMed
-
- Fong BP, Brackmann DE, Telischi FF. The long-term follow-up of drainage procedures for petrous apex cholesterol granulomas. Arch Otolaryngol Head Neck Surg. 1995;121:426–430. - PubMed
-
- Mosnier I, Cyna-Gorse F, Grayeli AB, Fraysse B, Martic C, Robier A, et al. Management of cholesterol granulomas of the petrous apex based on clinical and radiologic evaluation. Otol Neurotol. 2002;23:522–528. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
