

Bone loss after bariatric surgery: causes, consequences, and management
- PMID: 24622720
- PMCID: PMC4467779
- DOI: 10.1016/S2213-8587(13)70183-9
Bone loss after bariatric surgery: causes, consequences, and management
Abstract
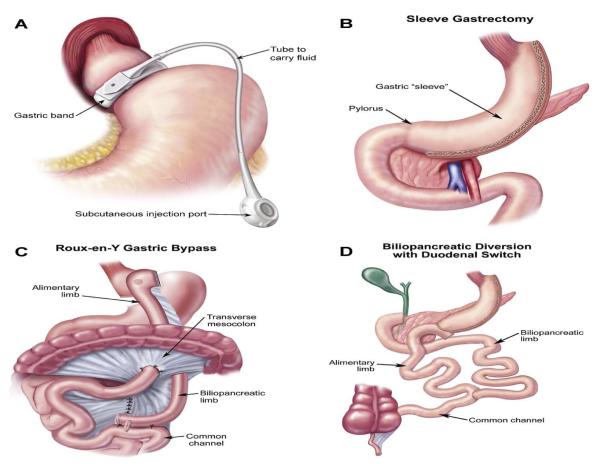
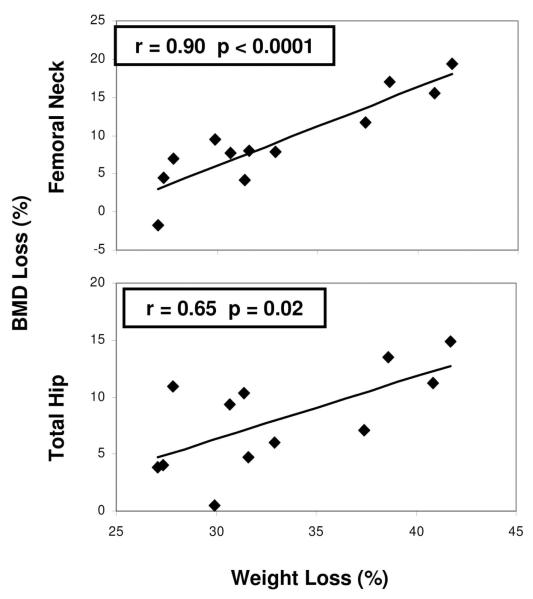
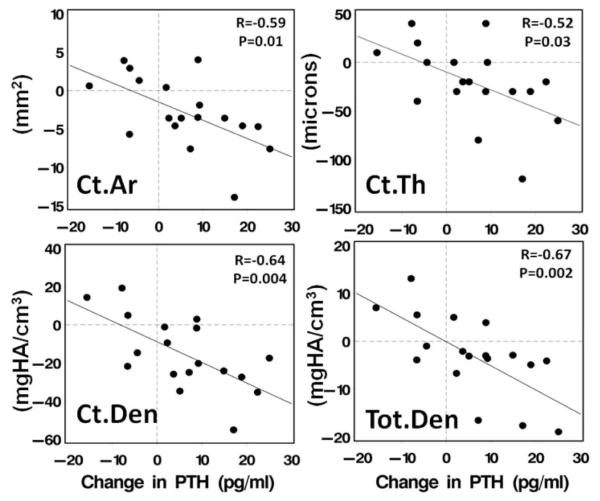
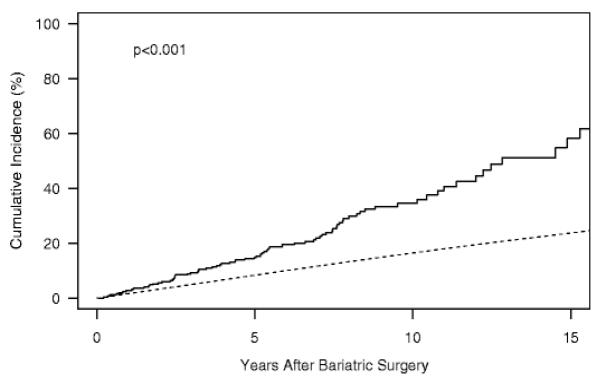
Bariatric surgery is an effective and increasingly common treatment for severe obesity and its many comorbidities. The side-effects of bariatric surgery can include detrimental effects on bone and mineral metabolism. Bone disease in patients who have had bariatric surgery is affected by preoperative abnormalities in bone and mineral metabolism related to severe obesity. Changes that arise after bariatric surgery are specific to procedure type: the most pronounced abnormalities in calciotropic hormones and bone loss are noted after procedures that result in the most malabsorption. The most consistent site for bone loss after all bariatric procedures is at the hip. There are limitations of dual-energy x-ray absorptiometry technology in this population, including artefact introduced by adipose tissue itself. Bone loss after bariatric surgery is probably multifactorial. Proposed mechanisms include skeletal unloading, abnormalities in calciotropic hormones, and changes in gut hormones. Few data for fracture risk in the bariatric population are available, and this is a crucial area for additional research. Treatment should be geared toward correction of nutritional deficiencies and study of bone mineral density in high-risk patients. We explore the skeletal response to bariatric surgery, potential mechanisms for changes, and strategies for management.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
References
-
- Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2013;9(2):159–91. - PubMed
-
- Buchwald H, Oien DM. Metabolic/bariatric surgery Worldwide 2008. Obes Surg. 2009;19(12):1605–11. - PubMed
-
- Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288(22):2793–6. - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes. N Engl J Med. 2012 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
