

Low intraoperative tidal volume ventilation with minimal PEEP is associated with increased mortality
- PMID: 24623057
- PMCID: PMC9585620
- DOI: 10.1093/bja/aeu054
Low intraoperative tidal volume ventilation with minimal PEEP is associated with increased mortality
Abstract
Background: Anaesthetists have traditionally ventilated patients' lungs with tidal volumes (TVs) between 10 and 15 ml kg(-1) of ideal body weight (IBW), without the use of PEEP. Over the past decade, influenced by the results of the Acute Respiratory Distress Syndrome Network trial, many anaesthetists have begun using lower TVs during surgery. It is unclear whether the benefits of low TV ventilation can be extended into the perioperative period.
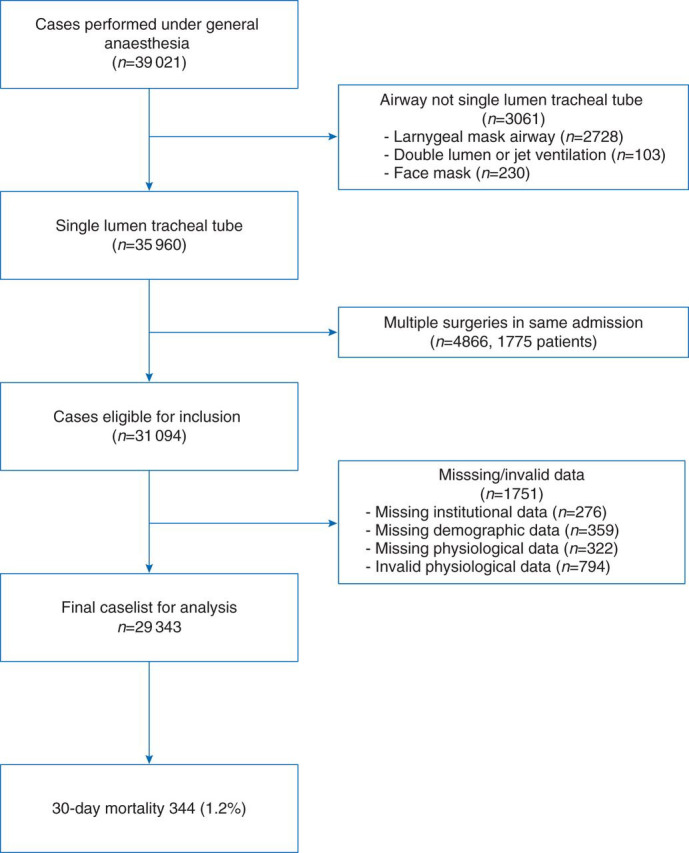
Methods: We reviewed the records of 29 343 patients who underwent general anaesthesia with mechanical ventilation between January 1, 2008 and December 31, 2011. We calculated TV kg(-1) IBW, PEEP, peak inspiratory pressure (PIP), and dynamic compliance. Cox regression analysis with propensity score matching was performed to examine the association between TV and 30-day mortality.
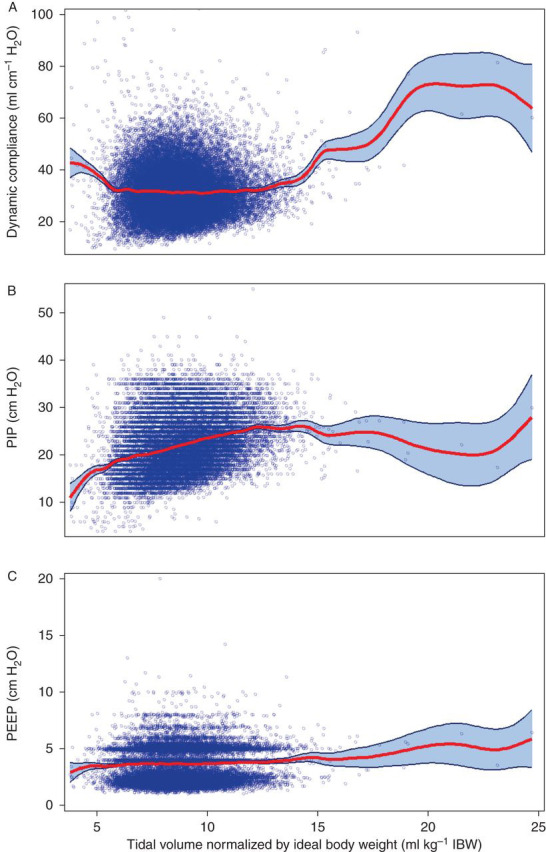
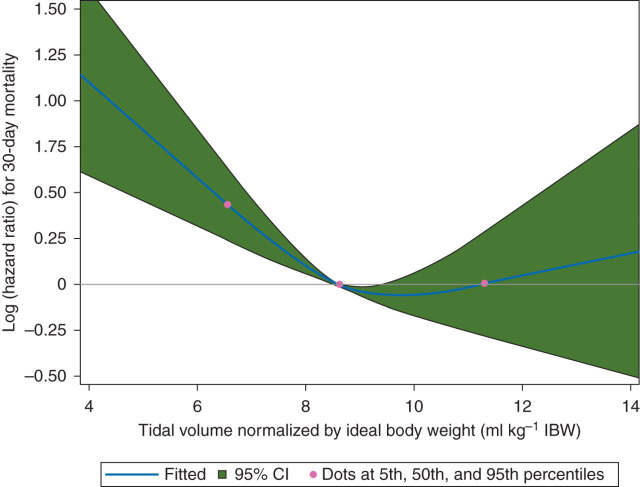
Results: Median TV was 8.6 [7.7-9.6] ml kg(-1) IBW with minimal PEEP [4.0 (2.2-5.0) cm H2O]. A significant reduction in TV occurred over the study period, from 9 ml kg(-1) IBW in 2008 to 8.3 ml kg(-1) IBW in 2011 (P=0.01). Low TV 6-8 ml kg(-1) IBW was associated with a significant increase in 30-day mortality vs TV 8-10 ml kg(-1) IBW: hazard ratio (HR) 1.6 [95% confidence interval (CI) [1.25-2.08], P=0.0002]. The association remained significant after matching: HR 1.63 [95% CI (1.22-2.18), P<0.001]. There was only a weak correlation between TV kg(-1) IBW and dynamic compliance (r=-0.006, P=0.31) and a weak-to-moderate correlation between TV kg(-1) IBW and PIP (r=0.32 P<0.0001).
Conclusions: Use of low intraoperative TV with minimal PEEP is associated with an increased risk of 30-day mortality.
Keywords: intraoperative care; pulmonary ventilation; tidal volume.
© The Author [2014]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
None declared.
Figures
Comment in
-
Low intraoperative tidal volume ventilation with minimal PEEP and postoperative morbidity and mortality.Br J Anaesth. 2015 Mar;114(3):520-1. doi: 10.1093/bja/aev011. Br J Anaesth. 2015. PMID: 25694556 No abstract available.
-
Low tidal volumes during intraoperative ventilation: Beneficial or Harmful?Br J Anaesth. 2015 Mar;114(3):521. doi: 10.1093/bja/aev007. Br J Anaesth. 2015. PMID: 25694557 No abstract available.
-
Reply from the authors.Br J Anaesth. 2015 Mar;114(3):522-3. doi: 10.1093/bja/aev008. Br J Anaesth. 2015. PMID: 25694558 No abstract available.
References
-
- Bendixen HH, Hedley-Whyte J, Laver MB. Impaired oxygenation in surgical patients during general anesthesia with controlled ventilation. A concept of atelectasis. N Engl J Med. 1963;269:991–996. - PubMed
-
- Brower RG, Matthay BMA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Choi G, Wolthuis EK, Bresser P, et al. Mechanical ventilation with lower tidal volumes and positive end-expiratory pressure prevents alveolar coagulation in patients without lung injury. Anesthesiology. 2006;105:689–695. - PubMed
-
- Wolthuis EK, Choi G, Dessing MC, et al. Mechanical ventilation with lower tidal volumes and positive end-expiratory pressure prevents pulmonary inflammation in patients without preexisting lung injury. Anesthesiology. 2007;108:46–54. - PubMed
-
- Blum JM, Fetterman DM, Park PK, Morris M, Rosenberg AL. A description of intraoperative ventilator management and ventilation strategies in hypoxic patients. Anesth Analg. 2010;110:1616–1622. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
