

Vascular risk factors, large-artery atheroma, and brain white matter hyperintensities
- PMID: 24623838
- PMCID: PMC4001185
- DOI: 10.1212/WNL.0000000000000312
Vascular risk factors, large-artery atheroma, and brain white matter hyperintensities
Abstract
Objective: To determine the magnitude of potentially causal relationships among vascular risk factors (VRFs), large-artery atheromatous disease (LAD), and cerebral white matter hyperintensities (WMH) in 2 prospective cohorts.
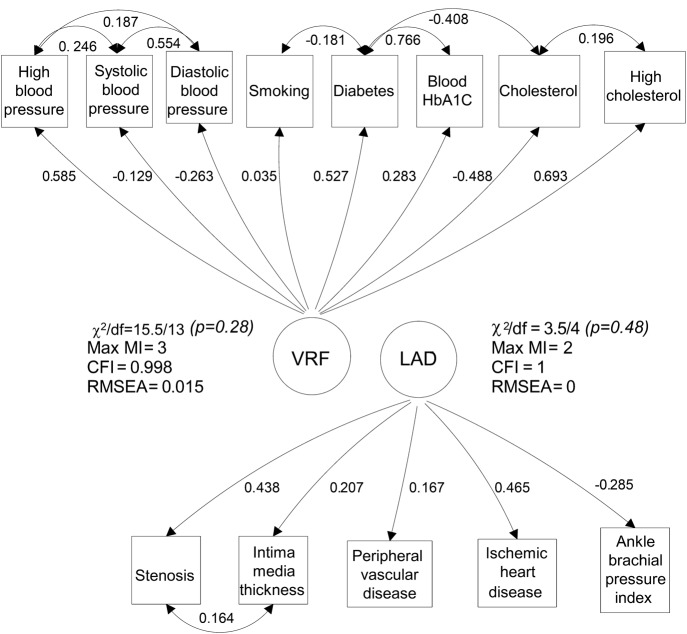
Methods: We assessed VRFs (history and measured variables), LAD (in carotid, coronary, and leg arteries), and WMH (on structural MRI, visual scores and volume) in: (a) community-dwelling older subjects of the Lothian Birth Cohort 1936, and (b) patients with recent nondisabling stroke. We analyzed correlations, developed structural equation models, and performed mediation analysis to test interrelationships among VRFs, LAD, and WMH.
Results: In subjects of the Lothian Birth Cohort 1936 (n = 881, mean age 72.5 years [SD ±0.7 years], 49% with hypertension, 33% with moderate/severe WMH), VRFs explained 70% of the LAD variance but only 1.4% to 2% of WMH variance, of which hypertension explained the most. In stroke patients (n = 257, mean age 74 years [SD ±11.6 years], 61% hypertensive, 43% moderate/severe WMH), VRFs explained only 0.1% of WMH variance. There was no direct association between LAD and WMH in either sample. The results were the same for all WMH measures used.
Conclusions: The small effect of VRFs and LAD on WMH suggests that WMH have a large "nonvascular," nonatheromatous etiology. VRF modification, although important, may be limited in preventing WMH and their stroke and dementia consequences. Investigation of, and interventions against, other suspected small-vessel disease mechanisms should be addressed.
Figures

References
-
- Baezner H, Blahak C, Poggesi A, et al. Association of gait and balance disorders with age-related white matter changes: the LADIS study. Neurology 2008;70:935–942 - PubMed
-
- Guo X, Pantoni L, Simoni M, et al. Blood pressure components and changes in relation to white matter lesions: a 32-year prospective population study. Hypertension 2009;54:57–62 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources