

Indications and interventional options for non-resectable tracheal stenosis
- PMID: 24624290
- PMCID: PMC3949180
- DOI: 10.3978/j.issn.2072-1439.2013.11.08
Indications and interventional options for non-resectable tracheal stenosis
Abstract
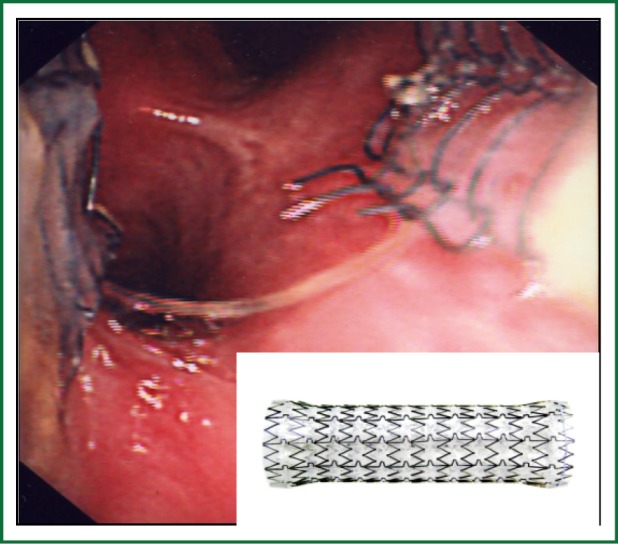
Non-specific presentation and normal examination findings in early disease often result in tracheal obstruction being overlooked as a diagnosis until patients present acutely. Once diagnosed, surgical options should be considered, but often patient co-morbidity necessitates other interventional options. Non-resectable tracheal stenosis can be successfully managed by interventional bronchoscopy, with therapeutic options including airway dilatation, local tissue destruction and airway stenting. There are common aspects to the management of tracheal obstruction, tracheomalacia and tracheal fistulae. This paper reviews the pathogenesis, presentation, investigation and management of tracheal disease, with a focus on tracheal obstruction and the role of endotracheal intervention in management.
Keywords: Airway stent; large airway obstruction; laser therapy; rigid bronchoscopy; tracheal stenosis.
Figures

References
-
- Whited RE. A prospective study of laryngotracheal sequelae in long-term intubation. Laryngoscope 1984;94:367-77 - PubMed
-
- Anand VK, Alemar G, Warren ET. Surgical considerations in tracheal stenosis. Laryngoscope 1992;102:237-43 - PubMed
-
- Grillo HC, Cooper JD, Geffin B, et al. A low-pressure cuff for tracheostomy tubes to minimize tracheal injury. A comparative clinical trial. J Thorac Cardiovasc Surg 1971;62:898-907 - PubMed
-
- Pearson FG, Andrews MJ. Detection and management of tracheal stenosis following cuffed tube tracheostomy. Ann Thorac Surg 1971;12:359-74 - PubMed
Publication types
LinkOut - more resources
Full Text Sources