

Visceral injury in electrical shock trauma: proposed guideline for the management of abdominal electrocution and literature review
- PMID: 24624308
- PMCID: PMC3945822
Visceral injury in electrical shock trauma: proposed guideline for the management of abdominal electrocution and literature review
Abstract
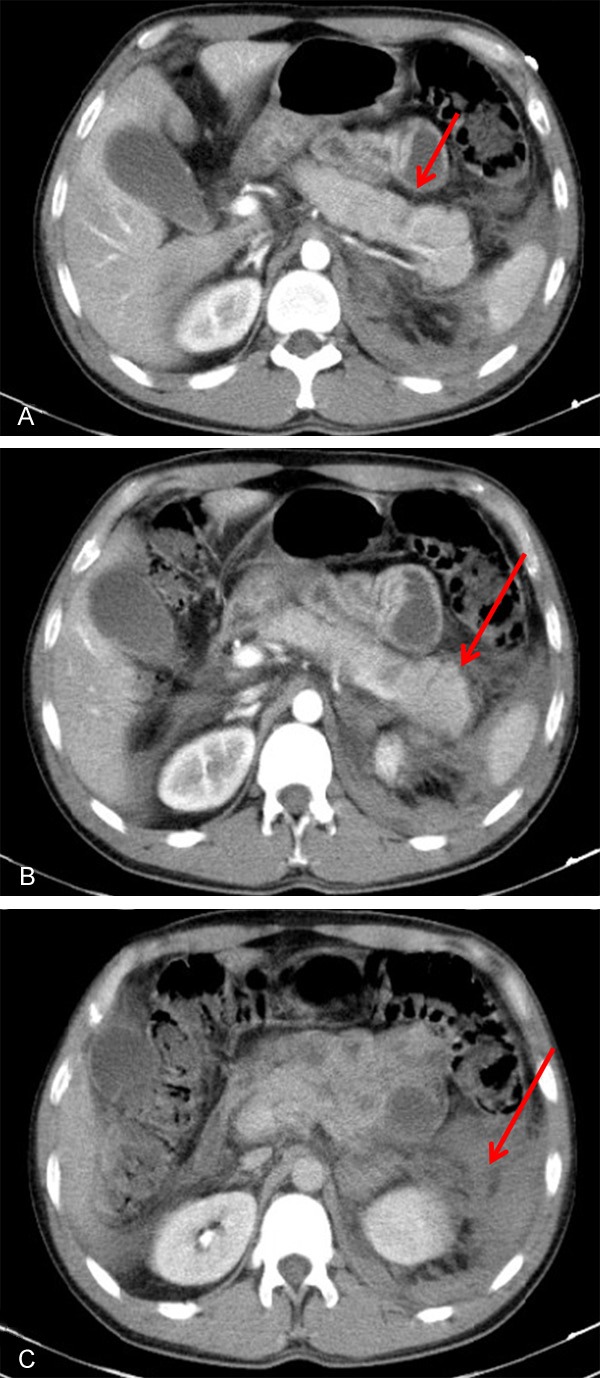
Victims of electrical burns account for approximately 5% of admissions to major burn centers. The first case of visceral injury caused by electrical burns was described in 1927 by Simonin, who reported perforation of the small intestine. Other rare cases were reported over the following years. The colon and small intestine were the organs most frequently affected. Less frequently involved organs were the heart, esophagus, stomach, pancreas, liver, gallbladder, lung, and kidney. We highlight the potential fatal visceral injuries after the electrical trauma. This study provides a review on this topic and proposes a management flowchart that should be adopted by the multidisciplinary team to treat these patients.
Conclusion: Visceral injuries are rare in electrical burns victims, but it can be severe and are associated with high rates of morbidity and mortality, sometimes requiring a more interventional approach.
Keywords: Electrical burn; electrical shock; pancreatic injuries; visceral injuries.
Figures



References
-
- Lee RC. Injury by electrical forces: pathophysiology, manifestations and therapy. Curr Probl Surg. 1997;34:677–764. - PubMed
-
- Esselman PC, Thombs BD, Magyar-Russell G, Fauerbach JA. Burn rehabilitation: state of the science. Am J Phys Med Rehabil. 2006;85:383–418. - PubMed
-
- Masanés MJ, Gourbiére E, Prudent J, Lioret N, Febvre M, Prévot S, Lebeau B. A high voltage electrical burn of lung parenchyma. Burns. 2000;26:659–63. - PubMed
-
- Arnoldo BD, Purdue GF. The diagnosis and management of electrical injuries. Hand Clin. 2009;25:469–79. - PubMed
-
- GourbieÁre E, Corbut JP, Brazin Y. Functional consequence of electrical injury. Electrical injury: a multidisciplinary approach to therapy, prevention and rehabilitation. Ann N Y Acad Sci. 1994;720:259–71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources