

Distribution of cardiovascular disease and retinopathy in patients with type 2 diabetes according to different classification systems for chronic kidney disease: a cross-sectional analysis of the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study
- PMID: 24624891
- PMCID: PMC4008155
- DOI: 10.1186/1475-2840-13-59
Distribution of cardiovascular disease and retinopathy in patients with type 2 diabetes according to different classification systems for chronic kidney disease: a cross-sectional analysis of the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study
Abstract
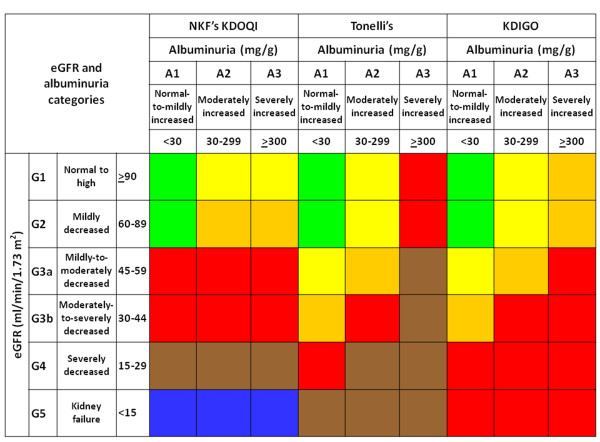
Background: The National Kidney Foundation's Kidney Disease Outcomes Quality Initiative (NKF's KDOQI) staging system for chronic kidney disease (CKD) is based primarily on estimated GFR (eGFR). This study aimed at assessing whether reclassification of subjects with type 2 diabetes using two recent classifications based on both eGFR and albuminuria, the Alberta Kidney Disease Network (AKDN) and the Kidney Disease: Improving Global Outcomes (KDIGO), provides a better definition of burden from cardiovascular disease (CVD) and diabetic retinopathy (DR) than the NKF's KDOQI classification.
Methods: This is a cross-sectional analysis of patients with type 2 diabetes (n = 15,773) from the Renal Insufficiency And Cardiovascular Events Italian Multicenter Study, consecutively visiting 19 Diabetes Clinics throughout Italy in years 2007-2008. Exclusion criteria were dialysis or renal transplantation. CKD was defined based on eGFR, as calculated from serum creatinine by the simplified Modification of Diet in Renal Disease Study equation, and albuminuria, as measured by immunonephelometry or immunoturbidimetry. DR was assessed by dilated fundoscopy. Prevalent CVD, total and by vascular bed, was assessed from medical history by recording previous documented major acute events.
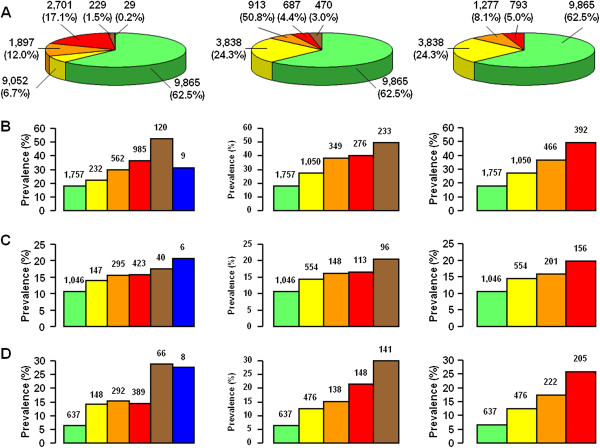
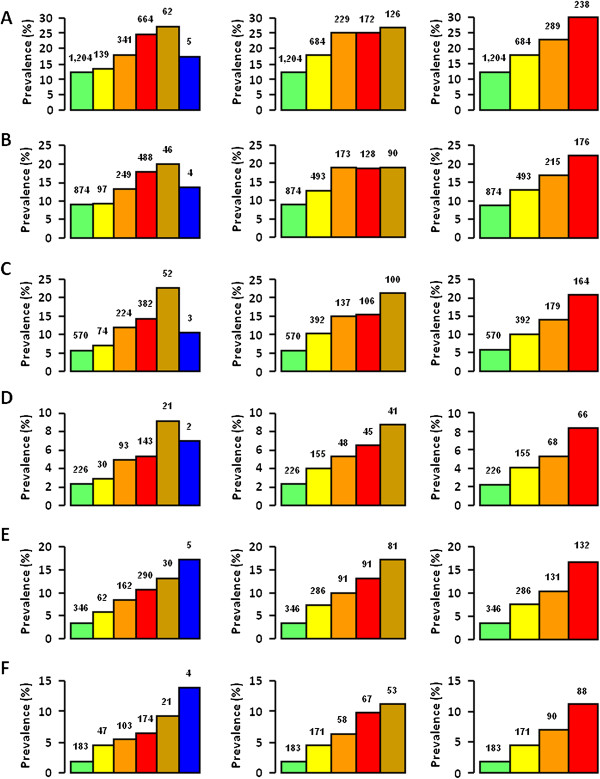
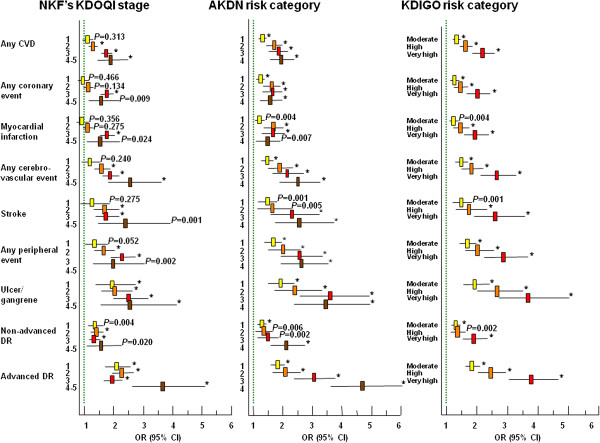
Results: Though prevalence of complications increased with increasing CKD severity with all three classifications, it differed significantly between NKF's KDOQI stages and AKDN or KDIGO risk categories. The AKDN and KDIGO systems resulted in appropriate reclassification of uncomplicated patients in the lowest risk categories and a more graded independent association with CVD and DR than the NKF's KDOQI classification. However, CVD, but not DR prevalence was higher in the lowest risk categories of the new classifications than in the lowest stages of the NKF's KDOQI, due to the inclusion of subjects with reduced eGFR without albuminuria. CVD prevalence differed also among eGFR and albuminuria categories grouped into AKDN and KDIGO risk category 1 and moderate, respectively, and to a lesser extent into higher risk categories.
Conclusions: Though the new systems perform better than the NKF's KDOQI in grading complications and identifying diabetic subjects without complications, they might underestimate CVD burden in patients assigned to lower risk categories and should be tested in large prospective studies.
Trial registration: ClinicalTrials.gov; NCT00715481.
Figures
References
-
- Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G. National Kidney Foundation: National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139:137–147. doi: 10.7326/0003-4819-139-2-200307150-00013. - DOI - PubMed
-
- Glassock RJ, Winearls C. An epidemic of chronic kidney disease: fact or fiction? Nephrol Dial Transplant. 2008;23:1117–1121. - PubMed
-
- Thomas MC, Macisaac RJ, Jerums G, Weekes A, Moran J, Shaw JE, Atkins RC. Nonalbuminuric renal impairment in type 2 diabetic patients and in the general population (national evaluation of the frequency of renal impairment cO-existing with NIDDM [NEFRON] 11) Diabetes Care. 2009;32:1497–1502. doi: 10.2337/dc08-2186. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
