

Cardiac fibroblast in development and wound healing
- PMID: 24625635
- PMCID: PMC4028446
- DOI: 10.1016/j.yjmcc.2014.02.017
Cardiac fibroblast in development and wound healing
Abstract
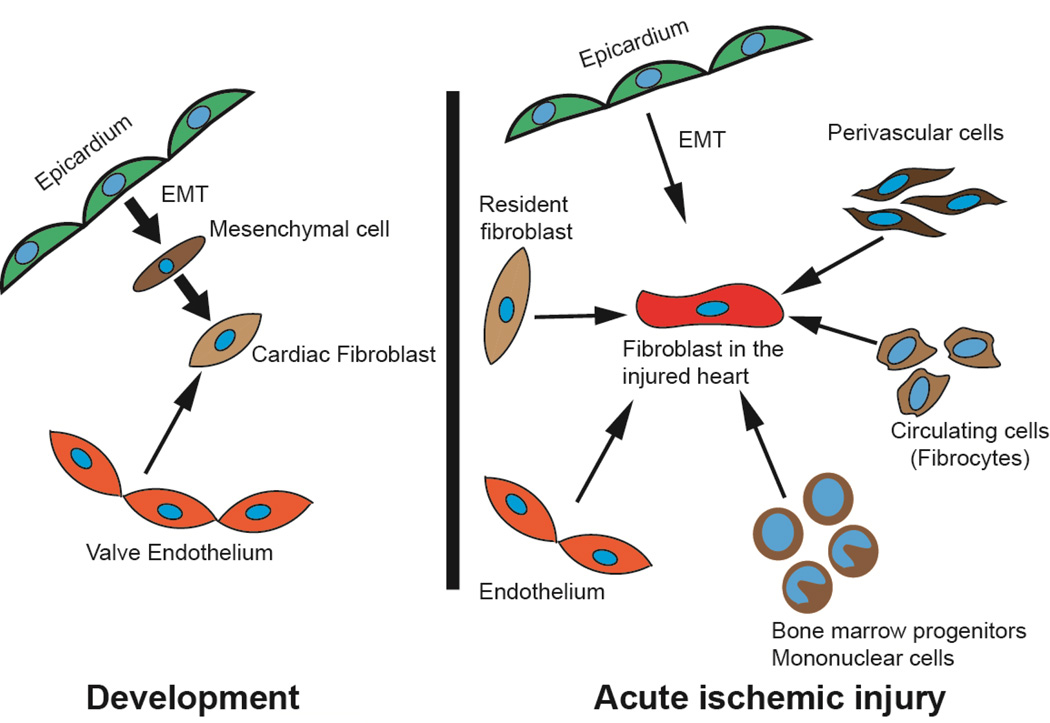
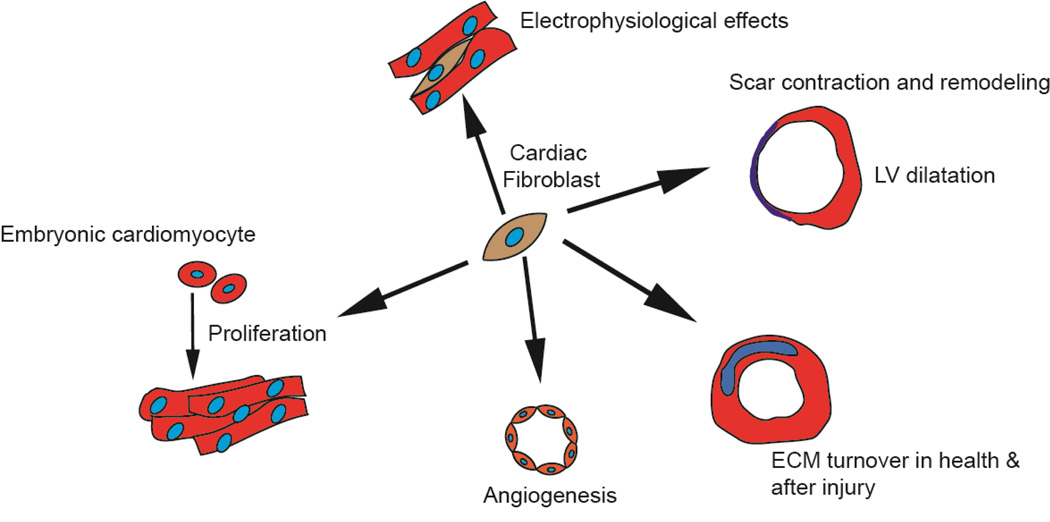
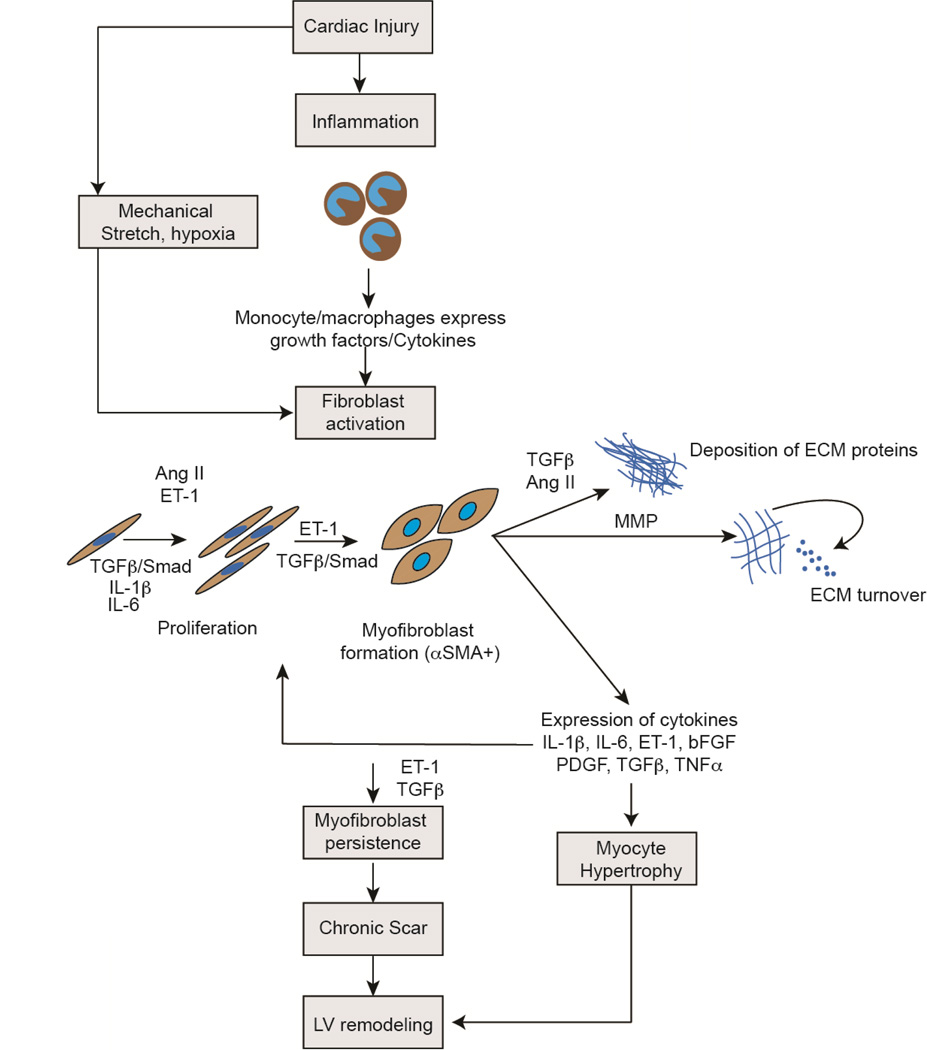
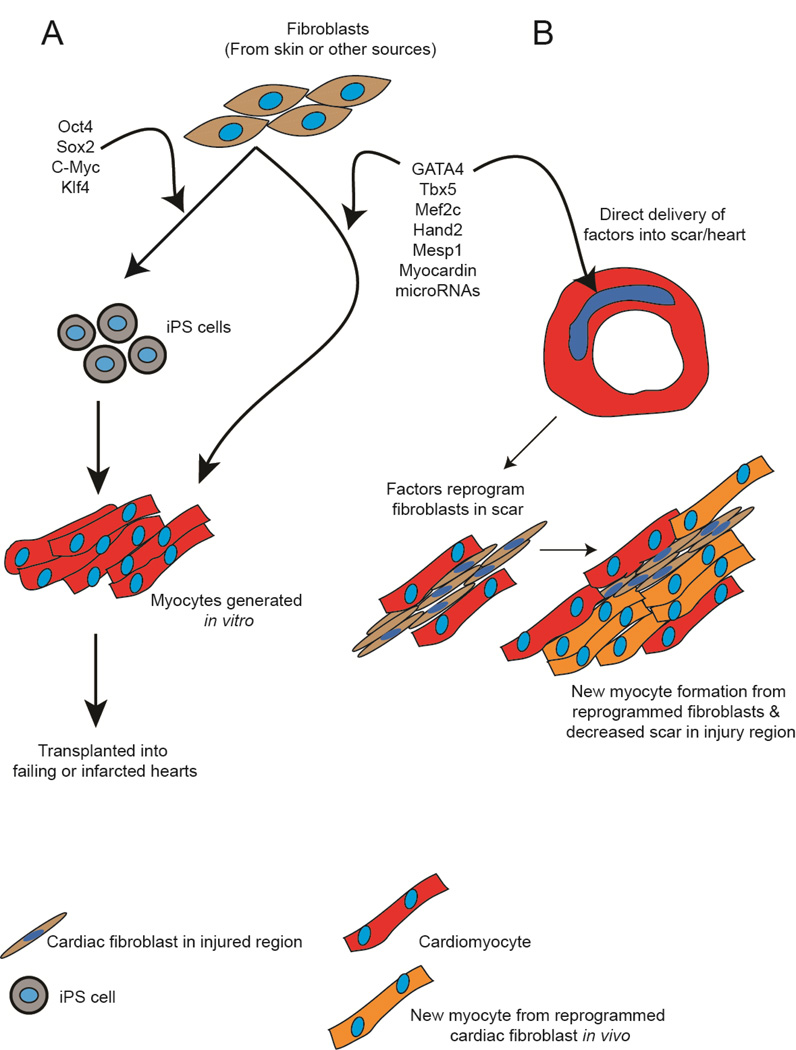
Cardiac fibroblasts are the most abundant cell type in the mammalian heart and comprise approximately two-thirds of the total number of cardiac cell types. During development, epicardial cells undergo epithelial-mesenchymal-transition to generate cardiac fibroblasts that subsequently migrate into the developing myocardium to become resident cardiac fibroblasts. Fibroblasts form a structural scaffold for the attachment of cardiac cell types during development, express growth factors and cytokines and regulate proliferation of embryonic cardiomyocytes. In post natal life, cardiac fibroblasts play a critical role in orchestrating an injury response. Fibroblast activation and proliferation early after cardiac injury are critical for maintaining cardiac integrity and function, while the persistence of fibroblasts long after injury leads to chronic scarring and adverse ventricular remodeling. In this review, we discuss the physiologic function of the fibroblast during cardiac development and wound healing, molecular mediators of activation that could be possible targets for drug development for fibrosis and finally the use of reprogramming technologies for reversing scar. This article is part of a Special Issue entitled "Myocyte-Fibroblast Signalling in Myocardium."
Keywords: Fibroblast; Fibrosis; Infarction; Remodeling; Repair; Wound healing.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
References
-
- Banerjee I, Fuseler JW, Price RL, Borg TK, Baudino TA. Determination of cell types and numbers during cardiac development in the neonatal and adult rat and mouse. Am J Physiol Heart Circ Physiol. 2007;293:H1883–H1891. - PubMed
-
- Zak R. Development and proliferative capacity of cardiac muscle cells. Circ Res. 1974;35(suppl II):17–26. - PubMed
