

Can ultrasound guidance reduce the risk of pneumothorax following thoracentesis?
- PMID: 24626264
- PMCID: PMC4075913
- DOI: 10.1590/S1806-37132014000100002
Can ultrasound guidance reduce the risk of pneumothorax following thoracentesis?
Abstract
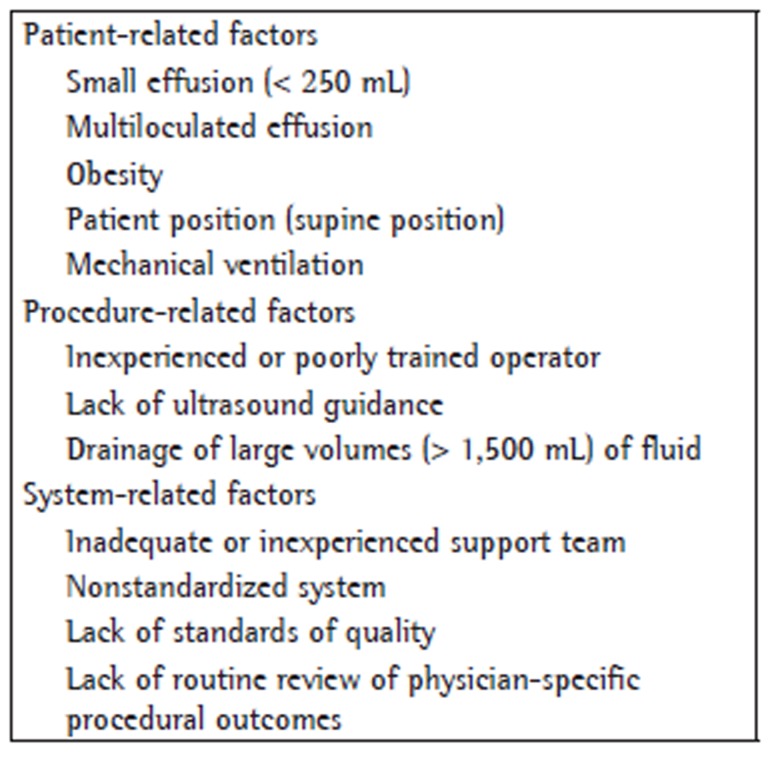
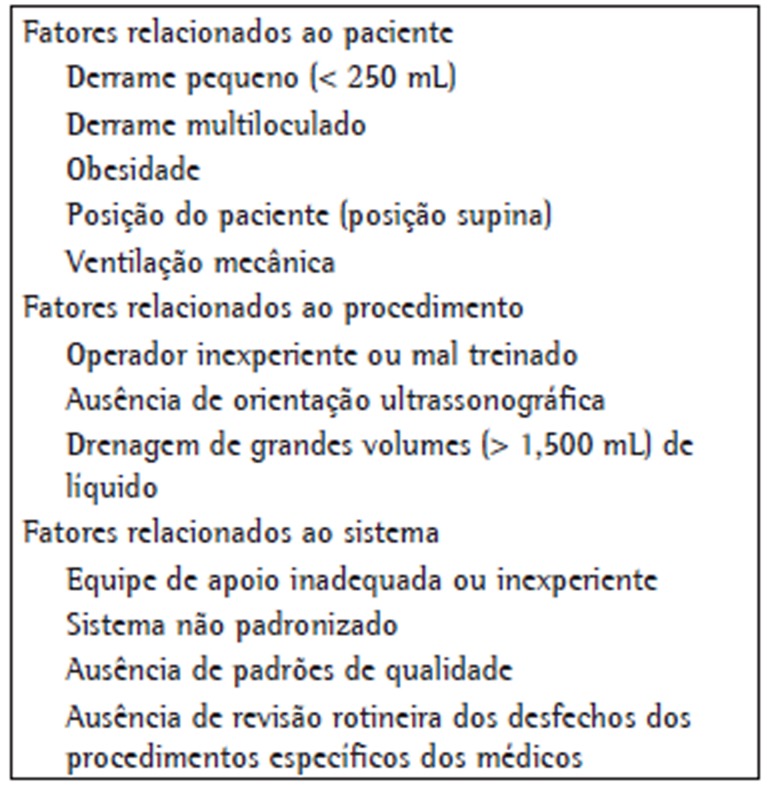
Objective: Thoracentesis is one of the bedside procedures most commonly associated with iatrogenic complications, particularly pneumothorax. Various risk factors for complications associated with thoracentesis have recently been identified, including an inexperienced operator; an inadequate or inexperienced support team; the lack of a standardized protocol; and the lack of ultrasound guidance. We sought to determine whether ultrasound-guided thoracentesis can reduce the risk of pneumothorax and improve outcomes (fewer procedures without fluid removal and greater volumes of fluid removed during the procedures). In our comparison of thoracentesis with and without ultrasound guidance, all procedures were performed by a team of expert pulmonologists, using the same standardized protocol in both conditions.
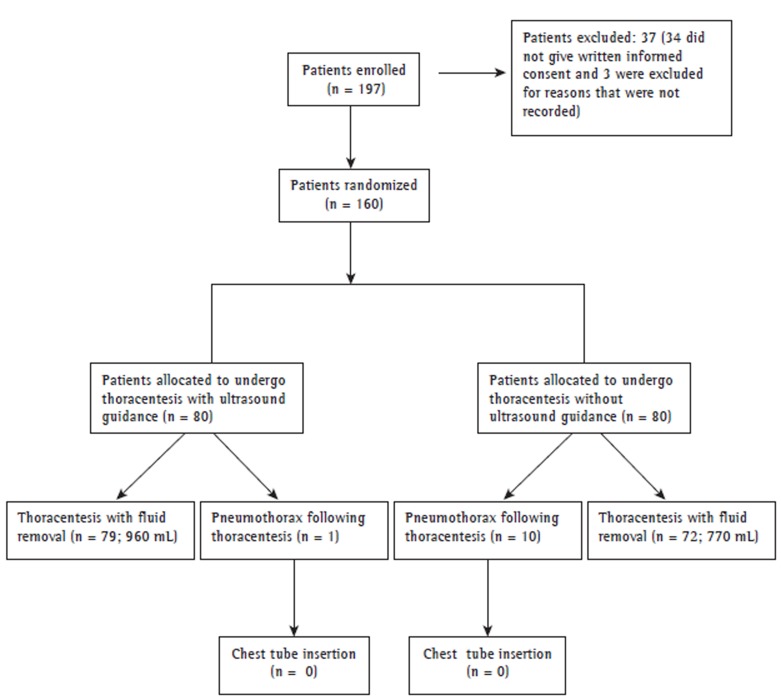
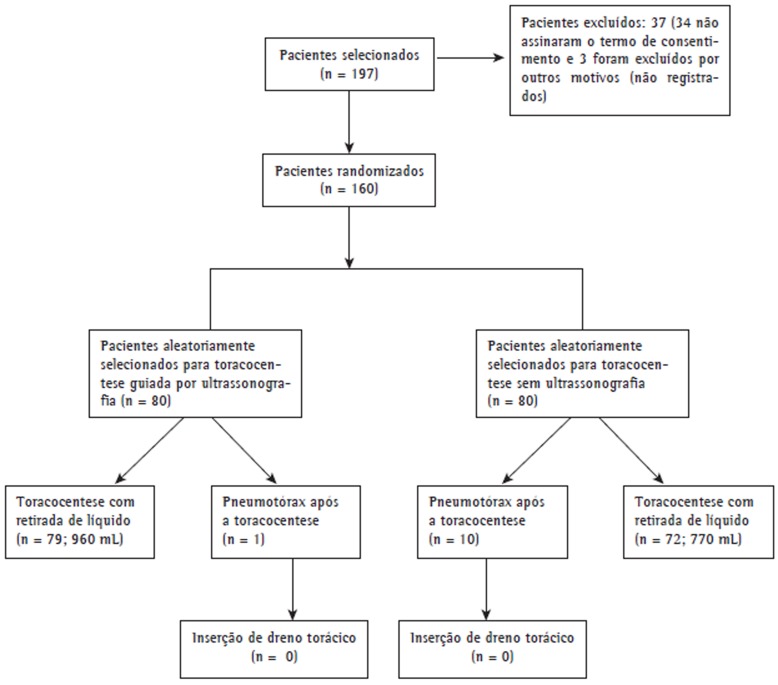
Methods: A total of 160 participants were randomly allocated to undergo thoracentesis with or without ultrasound guidance (n = 80 per group). The primary outcome was pneumothorax following thoracentesis. Secondary outcomes included the number of procedures without fluid removal and the volume of fluid drained during the procedure.
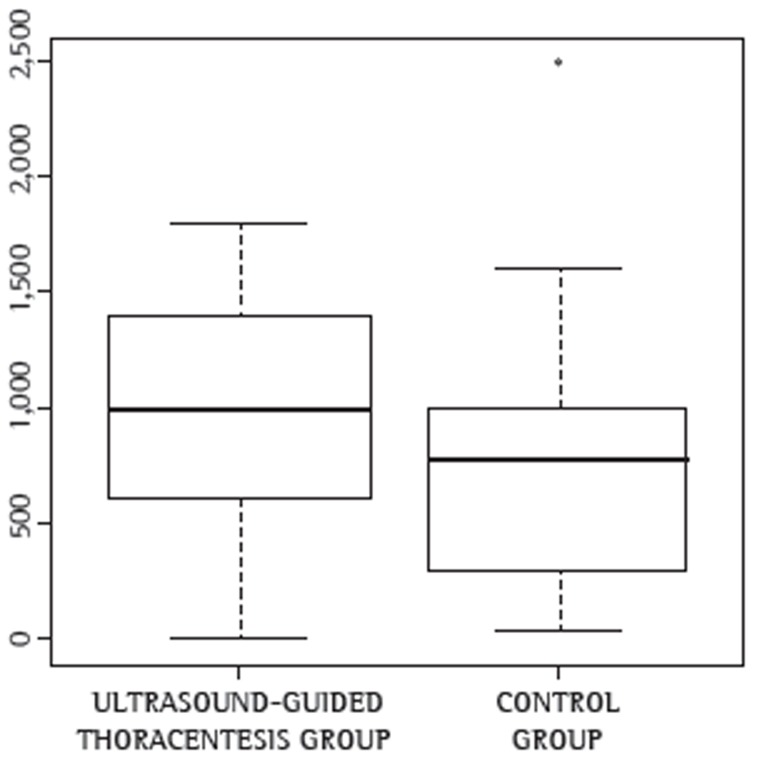
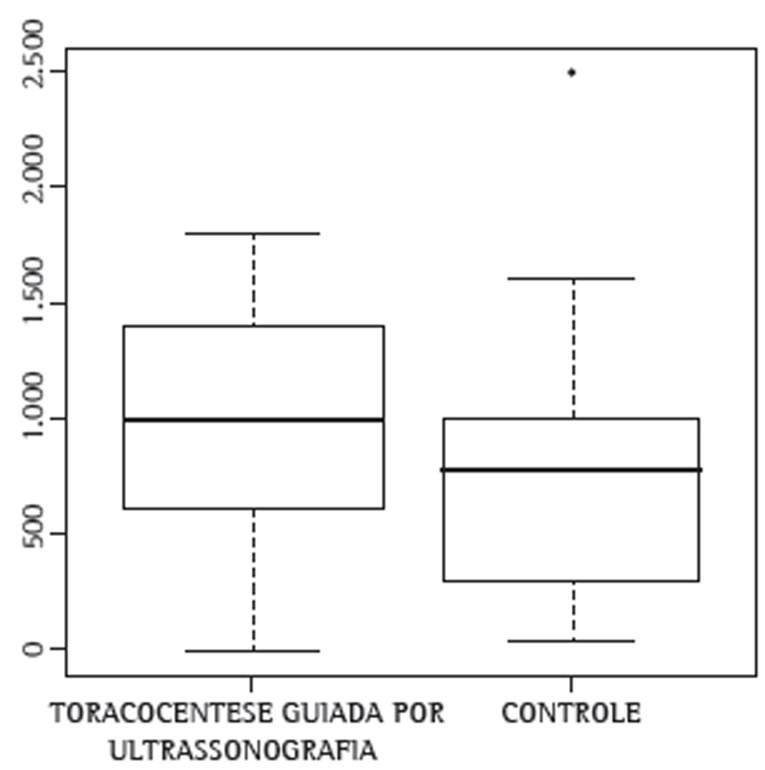
Results: Pneumothorax occurred in 1 of the 80 patients who underwent ultrasound-guided thoracentesis and in 10 of the 80 patients who underwent thoracentesis without ultrasound guidance, the difference being statistically significant (p = 0.009). Fluid was removed in 79 of the 80 procedures performed with ultrasound guidance and in 72 of the 80 procedures performed without it. The mean volume of fluid drained was larger during the former than during the latter (960 ± 500 mL vs. 770 ± 480 mL), the difference being statistically significant (p = 0.03).
Conclusions: Ultrasound guidance increases the yield of thoracentesis and reduces the risk of post-procedure pneumothorax. (Chinese Clinical Trial Registry identifier: ChiCTR-TRC-12002174 [http://www.chictr.org/en/]).
OBJETIVO:: Dentre os procedimentos realizados à beira do leito, a toracocentese é um dos mais comumente associados a complicações iatrogênicas, particularmente pneumotórax. Foram recentemente identificados vários fatores de risco de complicações associadas à toracocentese: a inexperiência do operador, a inadequação ou inexperiência da equipe de apoio, a ausência de um protocolo padronizado e a ausência de ultrassonografia para guiar o procedimento. Nosso objetivo foi determinar se a toracocentese guiada por ultrassonografia pode reduzir o risco de pneumotórax e melhorar os desfechos (menos procedimentos sem remoção de líquido e maior volume de líquido removido durante os procedimentos). Para compararmos a toracocentese guiada por ultrassonografia à toracocentese sem ultrassonografia, todos os procedimentos foram realizados pela mesma equipe de pneumologistas especialistas, os quais usaram o mesmo protocolo padronizado em ambas as condições.
MÉTODOS:: Cento e sessenta pacientes foram aleatoriamente divididos em dois grupos: toracocentese guiada por ultrassonografia e toracocentese sem ultrassonografia (n = 80 por grupo). O desfecho primário foi pneumotórax após a toracocentese. Os desfechos secundários foram o número de procedimentos sem remoção de líquido e o volume de líquido drenado durante o procedimento.
RESULTADOS:: Houve pneumotórax em 1 dos 80 pacientes submetidos a toracocentese guiada por ultrassonografia e em 10 dos 80 submetidos a toracocentese sem ultrassonografia; a diferença foi estatisticamente significante (p = 0,009). Líquido foi removido em 79 dos 80 procedimentos guiados por ultrassonografia e em 72 dos 80 que não o foram. A média do volume de líquido drenado foi maior nos procedimentos guiados por ultrassonografia do que naqueles que não o foram (960 ± 500 mL vs. 770 ± 480 mL); a diferença foi estatisticamente significante (p = 0,03).
CONCLUSÕES:: A ultrassonografia aumenta o rendimento da toracocentese e reduz o risco de pneumotórax após o procedimento. (Chinese Clinical Trial Registry identifier: ChiCTR-TRC-12002174 [http://www.chictr.org/en/])
Figures
Comment in
-
Lung ultrasound in the evaluation of pleural effusion.J Bras Pneumol. 2014 Jan-Feb;40(1):1-5. doi: 10.1590/S1806-37132014000100001. J Bras Pneumol. 2014. PMID: 24626263 Free PMC article. No abstract available.
References
-
- Light RW. Clinical practice. Pleural effusion. N Engl J Med. 2002;346(25):1971–1977. http://dx.doi.org/10.1056/NEJMcp010731 - DOI - PubMed
-
- Daniels CE, Ryu JH. Improving the safety of thoracentesis. Curr Opin Pulm Med. 2011;17(4):232–236. http://dx.doi.org/10.1097/MCP.0b013e328345160b - DOI - PubMed
-
- Gordon CE, Feller-Kopman D, Balk EM, Smetana GW. Pneumothorax following thoracentesis: a systematic review and meta-analysis. Arch Intern Med. 2010;170(4):332–339. http://dx.doi.org/10.1001/archinternmed.2009.548 - DOI - PubMed
-
- Duncan DR, Morgenthaler TI, Ryu JH, Daniels CE. Reducing iatrogenic risk in thoracentesis: establishing best practice via experiential training in a zero-risk environment. Chest. 2009;135(5):1315–1320. http://dx.doi.org/10.1378/chest.08-1227 - DOI - PubMed
-
- Havelock T, Teoh R, Laws D, Gleeson F, BTS Pleural Disease Guideline Group Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii61–ii76. http://dx.doi.org/10.1136/thx.2010.137026 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
