

Health and economic benefits of improved injury prevention and trauma care worldwide
- PMID: 24626472
- PMCID: PMC3953529
- DOI: 10.1371/journal.pone.0091862
Health and economic benefits of improved injury prevention and trauma care worldwide
Abstract
Objectives: Injury is a significant source of morbidity and mortality worldwide, and often disproportionately affects younger, more productive members of society. While many have made the case for improved injury prevention and trauma care, health system development in low- and middle-income countries is often limited by resources. This study aims to determine the economic benefit of improved injury prevention and trauma care in low- and middle-income countries.
Methods: This study uses existing data on injury mortality worldwide from the 2010 Global Burden of Disease Study to estimate the number of lives that could be saved if injury mortality rates in low- and middle-income countries could be reduced to rates in high-income countries. Using economic modeling--through the human capital approach and the value of a statistical life approach--the study then demonstrates the associated economic benefit of these lives saved.
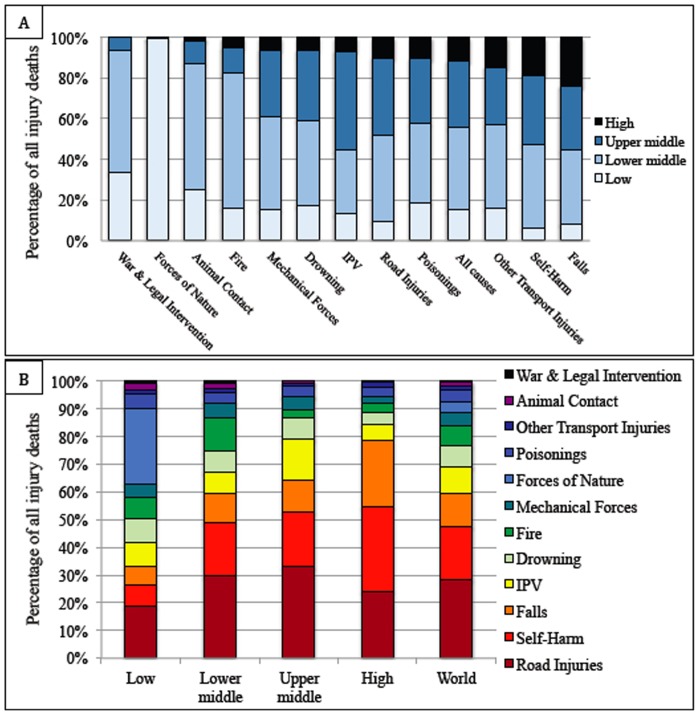
Results: 88 percent of injury-related deaths occur in low- and middle-income countries. If injury mortality rates in low- and middle-income countries were reduced to rates in high-income countries, 2,117,500 lives could be saved per year. This would result in between 49 million and 52 million disability adjusted life years averted per year, with discounting and age weighting. Using the human capital approach, the associated economic benefit of reducing mortality rates ranges from $245 to $261 billion with discounting and age weighting. Using the value of a statistical life approach, the benefit is between 758 and 786 billion dollars per year.
Conclusions: Reducing injury mortality in low- and middle-income countries could save over 2 million lives per year and provide significant economic benefit globally. Further investments in trauma care and injury prevention are needed.
Conflict of interest statement
Figures
References
-
- Debas HT, Gosselin R, McCord C, Thind A (2006) Surgery. In: Jamison DT, editor. Disease control priorities in developing countries. 2 ed. New York: Oxford University Press; pp. 1245–60.
-
- Lopez A, Mathers C, Ezzati M, Jamison D, Murray C, editors. (2006) Global burden of disease and risk factors. New York, NY: The World Bank and Oxford University Press. - PubMed
-
- Patton GC, Coffey C, Sawyer SM, Viner RM, Haller DM, et al. (2009) Global patterns of mortality in young people: a systematic analysis of population health data. Lancet 374: 881–892. - PubMed
-
- Murray C, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2197–2223. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
