

Acquired hyperpigmentations
- PMID: 24626644
- PMCID: PMC3938350
- DOI: 10.1590/abd1806-4841.20142353
Acquired hyperpigmentations
Abstract
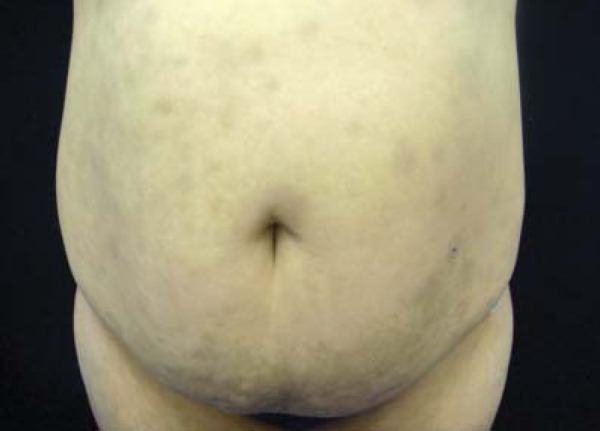
Cutaneous hyperpigmentations are frequent complaints, motivating around 8.5% of all dermatological consultations in our country. They can be congenital, with different patterns of inheritance, or acquired in consequence of skin problems, systemic diseases or secondary to environmental factors. The vast majority of them are linked to alterations on the pigment melanin, induced by different mechanisms. This review will focus on the major acquired hyperpigmentations associated with increased melanin, reviewing their mechanisms of action and possible preventive measures. Particularly prominent aspects of diagnosis and therapy will be emphasized, with focus on melasma, post-inflammatory hyperpigmentation, periorbital pigmentation, dermatosis papulosa nigra, phytophotodermatoses, flagellate dermatosis, erythema dyschromicum perstans, cervical poikiloderma (Poikiloderma of Civatte), acanthosis nigricans, cutaneous amyloidosis and reticulated confluent dermatitis.
Conflict of interest statement
Conflict of Interest: None.
Figures










References
-
- Sbd.org Censo Dermatologico da SBD. Brazilian Society of Dermatology Web page - Dermatological census. [Acesso 1 Dez. 2012]. [Internet] Disponível em: http://www.sbd.org.br/down/censo_dermatologico2006pdf2012.
-
- Sanchez NP, Pathak MA, Sato S, Fitzpatrick TB, Sanchez JL, Mihm MC., Jr Melasma: a clinical, light microscopic, ultrastructural, and immunofluorescence study. J Am Acad Dermatol. 1981;4:698–710. - PubMed
-
- Ritter CG, Fiss DV, Borges da Costa JA, de Carvalho RR, Bauermann G, Cestari TF. Extra-facial melasma: clinical, histopathological, and immunohistochemical case-control study. J Eur Acad Dermatol Venereol. 2013;27:1088–1094. - PubMed
-
- Taylor SC. Epidemiology of skin diseases in ethnic populations. Dermatol Clin. 2003;21:601–607. - PubMed
-
- Tamega Ade A, Miot LD, Bonfietti C, Gige TC, Marques ME, Miot HA. Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women. J Eur Acad Dermatol Venereol. 2013;27:151–156. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases