

An official American Thoracic Society clinical practice guideline: diagnosis, risk stratification, and management of pulmonary hypertension of sickle cell disease
- PMID: 24628312
- PMCID: PMC3983842
- DOI: 10.1164/rccm.201401-0065ST
An official American Thoracic Society clinical practice guideline: diagnosis, risk stratification, and management of pulmonary hypertension of sickle cell disease
Abstract
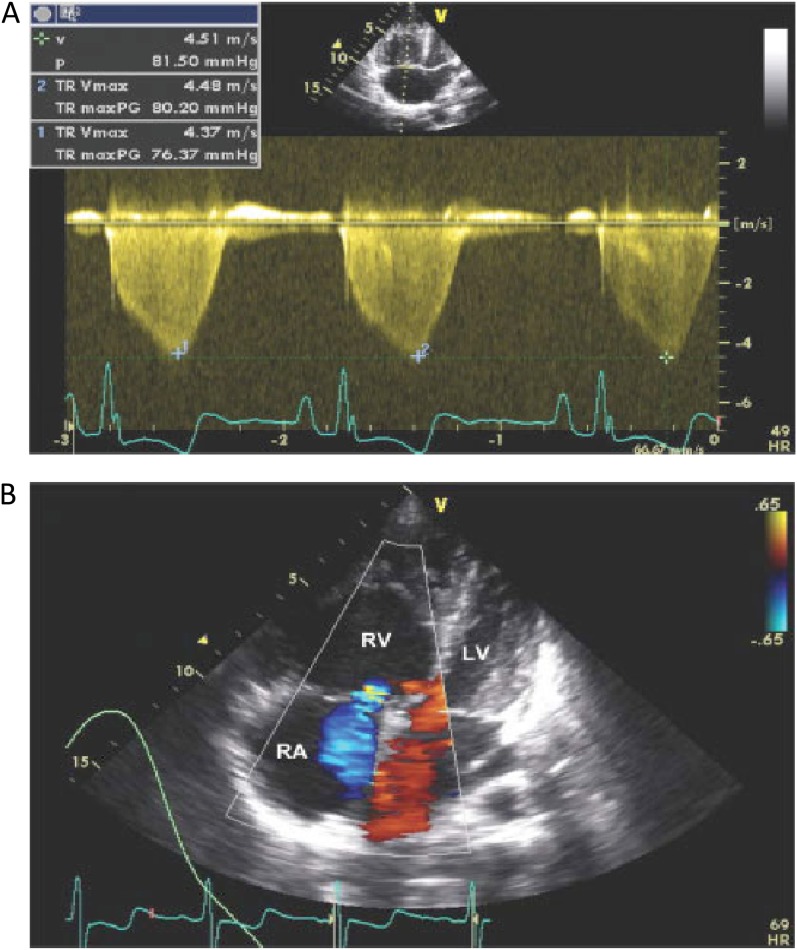
Background: In adults with sickle cell disease (SCD), an increased tricuspid regurgitant velocity (TRV) measured by Doppler echocardiography, an increased serum N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level, and pulmonary hypertension (PH) diagnosed by right heart catheterization (RHC) are independent risk factors for mortality.
Methods: A multidisciplinary committee was formed by clinician-investigators experienced in the management of patients with PH and/or SCD. Clinically important questions were posed, related evidence was appraised, and questions were answered with evidence-based recommendations. Target audiences include all clinicians who take care of patients with SCD.
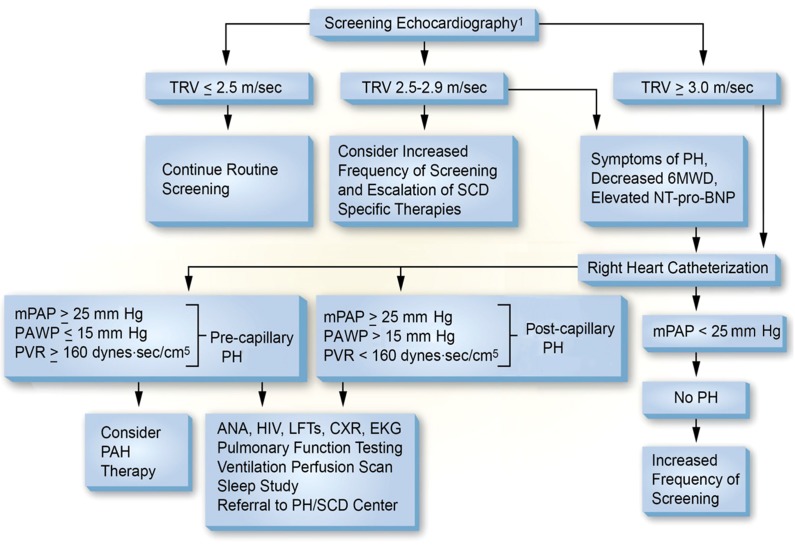
Results: Mortality risk stratification guides decision making. An increased risk for mortality is defined as a TRV equal to or greater than 2.5 m/second, an NT-pro-BNP level equal to or greater than 160 pg/ml, or RHC-confirmed PH. For patients identified as having increased mortality risk, we make a strong recommendation for hydroxyurea as first-line therapy and a weak recommendation for chronic transfusions as an alternative therapy. For all patients with SCD with elevated TRV alone or elevated NT-pro-BNP alone, and for patients with SCD with RHC-confirmed PH with elevated pulmonary artery wedge pressure and low pulmonary vascular resistance, we make a strong recommendation against PAH-specific therapy. However, for select patients with SCD with RHC-confirmed PH who have elevated pulmonary vascular resistance and normal pulmonary capillary wedge pressure, we make a weak recommendation for either prostacyclin agonist or endothelin receptor antagonist therapy and a strong recommendation against phosphodiesterase-5 inhibitor therapy.
Conclusions: Evidence-based recommendations for the management of patients with SCD with increased mortality risk are provided, but will require frequent reassessment and updating.
Figures
Comment in
-
Practice guideline for pulmonary hypertension in sickle cell: direct evidence needed before universal adoption.Am J Respir Crit Care Med. 2014 Jul 15;190(2):237-8. doi: 10.1164/rccm.201404-0640LE. Am J Respir Crit Care Med. 2014. PMID: 25025359 No abstract available.
-
Reply: Practice guideline for pulmonary hypertension in sickle cell: direct evidence needed before universal adoption.Am J Respir Crit Care Med. 2014 Jul 15;190(2):238-40. doi: 10.1164/rccm.201404-0733LE. Am J Respir Crit Care Med. 2014. PMID: 25025360 Free PMC article. No abstract available.
References
-
- Parent F, Bachir D, Inamo J, Lionnet F, Driss F, Loko G, Habibi A, Bennani S, Savale L, Adnot S, et al. A hemodynamic study of pulmonary hypertension in sickle cell disease. N Engl J Med. 2011;365:44–53. - PubMed
-
- Fonseca GH, Souza R, Salemi VC, Jardim CV, Gualandro SF. Pulmonary hypertension diagnosed by right heart catheterization in sickle cell disease. Eur Respir J. 2011 - PubMed
-
- Gladwin MT, Sachdev V, Jison ML, Shizukuda Y, Plehn JF, Minter K, Brown B, Coles WA, Nichols JS, Ernst I, et al. Pulmonary hypertension as a risk factor for death in patients with sickle cell disease. N Engl J Med. 2004;350:886–895. - PubMed
-
- Ataga KI, Moore CG, Jones S, Olajide O, Strayhorn D, Hinderliter A, Orringer EP. Pulmonary hypertension in patients with sickle cell disease: a longitudinal study. Br J Haematol. 2006;134:109–115. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials