

Bevacizumab plus octreotide and metronomic capecitabine in patients with metastatic well-to-moderately differentiated neuroendocrine tumors: the XELBEVOCT study
- PMID: 24628963
- PMCID: PMC3996907
- DOI: 10.1186/1471-2407-14-184
Bevacizumab plus octreotide and metronomic capecitabine in patients with metastatic well-to-moderately differentiated neuroendocrine tumors: the XELBEVOCT study
Abstract
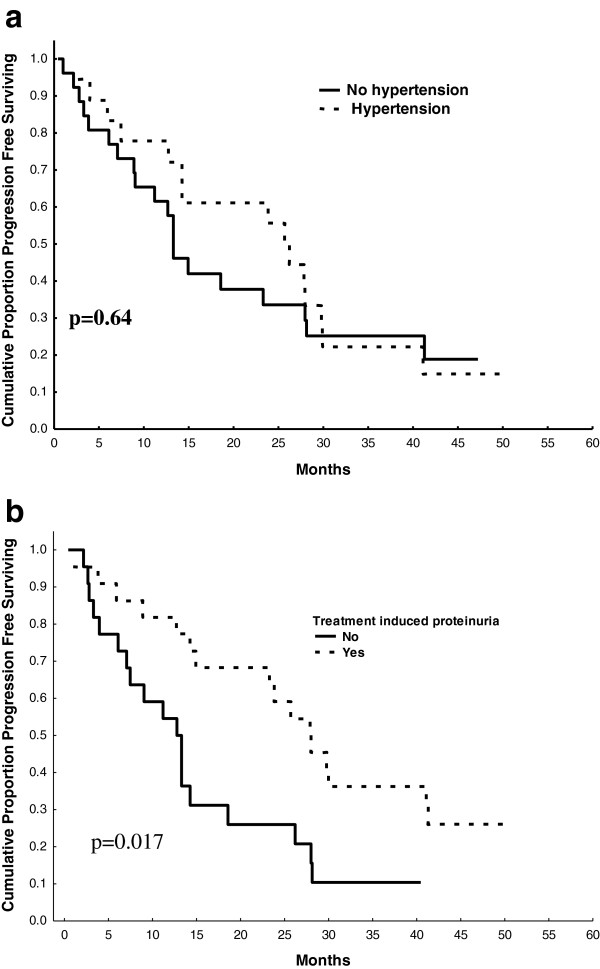
Background: We assessed the activity and toxicity of the XELBEVOCT regimen in patients with metastatic well-to-moderately differentiated neuroendocrine neoplasms (WMD-NEN). Ancillary studies evaluated hypertension, proteinuria, and vascular endothelial growth factor (VEGF) polymorphisms in predicting progression-free survival (PFS) and the predictive role of serum vitamin D in progression-free survival and proteinuria onset.
Methods: This prospective phase 2 study included 45 patients with WMD-NEN arising from various primary sites. The treatment regimen was octreotide long-acting release (LAR), 20 mg monthly, metronomic capecitabine, 2000 mg/daily, and intravenous bevacizumab, 5 mg/kg every 2 weeks, without interruption for 9 months. Bevacizumab was continued until disease progression.
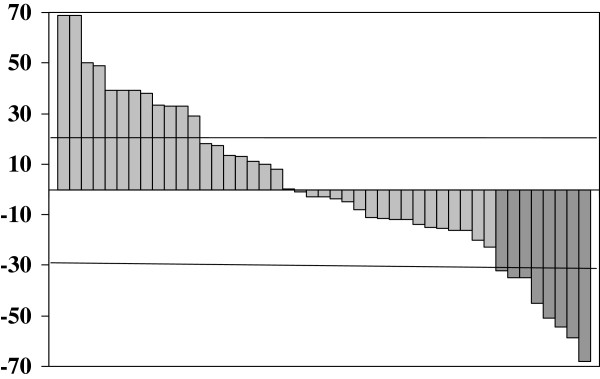
Results: Partial response was obtained in 8 patients (17.8%, 95% confidence interval [CI], 6.4%-28.2%); tumor response was more frequent in pancreatic than in non-pancreatic malignancies. The median PFS was 14.9 months; median overall survival was not attained. Biochemical and symptomatic responses were observed in 52.9% and 82.3% of cases, respectively. The treatment was well tolerated. Grade 3 toxicities included hand and foot syndrome (11.1%), proteinuria (4.4%), and renal toxicity (2.2%). Proteinuria (all grades) was correlated with longer PFS (p = 0.017). There was an inverse relationship between proteinuria and vitamin D levels. VEGF polymorphisms were not associated with patient outcome.
Conclusion: The XELBEVOCT regimen is active and well tolerated in patients with metastatic WMD-NEN. Proteinuria correlated with hypovitaminosis D status and was the best predictive factor of treatment efficacy.
Trial registration: Trial registration number NCT01203306.
Figures

References
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. Tumors of the Digestive System. World Health Organization Classification of Tumours. Pathology and Genetics. Lyon: IARC Press; 2010.
-
- Travis WD, Brambilla E, Muller-Hermelink HK, Harris CC. Tumours of the Lung, Pleura, Thymus and Heart. World Health Organization Classification Tumours. Pathology and Genetics 2004. Lyon: IARC Press; 2004.
-
- Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, Thakker RV, de Herder WW, Thakker RV, Caplin M, Delle Fave G, Kaltsas GA, Krenning EP, Moss SF, Nilsson O, Rindi G, Salazar R, Ruszniewski P, Sundin A. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9(1):61–72. doi: 10.1016/S1470-2045(07)70410-2. - DOI - PubMed
-
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, Abdalla EK, Fleming JB, Vauthey JN, Rashid A, Evans DB. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;18:3063–3072. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
