

Calorie intake and patient outcomes in severe acute kidney injury: findings from The Randomized Evaluation of Normal vs. Augmented Level of Replacement Therapy (RENAL) study trial
- PMID: 24629036
- PMCID: PMC4057152
- DOI: 10.1186/cc13767
Calorie intake and patient outcomes in severe acute kidney injury: findings from The Randomized Evaluation of Normal vs. Augmented Level of Replacement Therapy (RENAL) study trial
Abstract
Introduction: Current practice in the delivery of caloric intake (DCI) in patients with severe acute kidney injury (AKI) receiving renal replacement therapy (RRT) is unknown. We aimed to describe calorie administration in patients enrolled in the Randomized Evaluation of Normal vs. Augmented Level of Replacement Therapy (RENAL) study and to assess the association between DCI and clinical outcomes.
Methods: We performed a secondary analysis in 1456 patients from the RENAL trial. We measured the dose and evolution of DCI during treatment and analyzed its association with major clinical outcomes using multivariable logistic regression, Cox proportional hazards models, and time adjusted models.
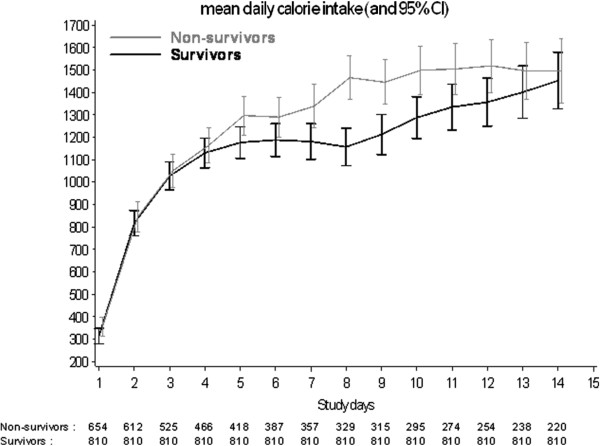
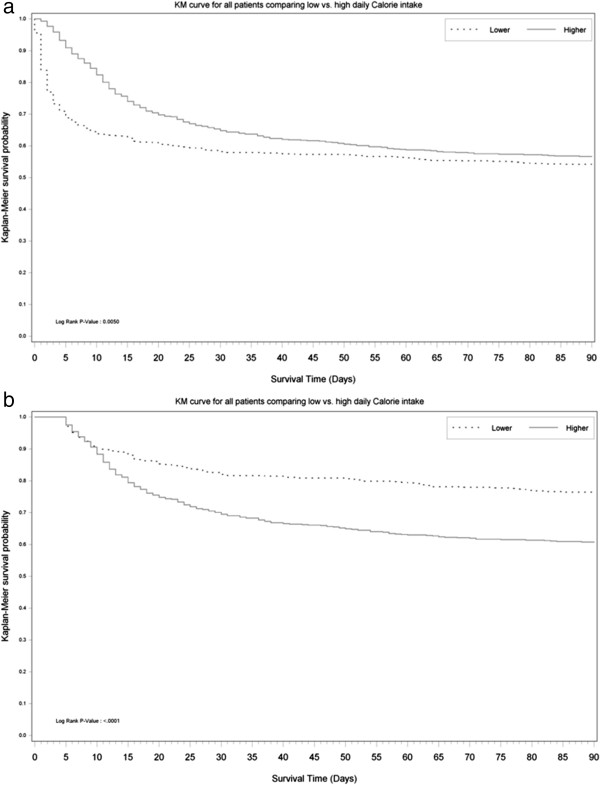
Results: Overall, mean DCI during treatment in ICU was low at only 10.9 ± 9 Kcal/kg/day for non-survivors and 11 ± 9 Kcal/kg/day for survivors. Among patients with a lower DCI (below the median) 334 of 729 (45.8%) had died at 90-days after randomization compared with 316 of 727 (43.3%) patients with a higher DCI (above the median) (P = 0.34). On multivariable logistic regression analysis, mean DCI carried an odds ratio of 0.95 (95% confidence interval (CI): 0.91-1.00; P = 0.06) per 100 Kcal increase for 90-day mortality. DCI was not associated with significant differences in renal replacement (RRT) free days, mechanical ventilation free days, ICU free days and hospital free days. These findings remained essentially unaltered after time adjusted analysis and Cox proportional hazards modeling.
Conclusions: In the RENAL study, mean DCI was low. Within the limits of such low caloric intake, greater DCI was not associated with improved clinical outcomes.
Trial registration: ClinicalTrials.gov number, NCT00221013.
Figures
Comment in
-
The nutritional energy to clinical outcome relation revisited.Crit Care. 2014 May 7;18(3):140. doi: 10.1186/cc13861. Crit Care. 2014. PMID: 25032513 Free PMC article.
References
-
- McClave SA, Martindale RG, Vanek VW, McCarthy M, Roberts P, Taylor B, Ochoa JB, Napolitano L, Cresci G. A.S.P.E.N. Board of Directors; American College of Critical Care Medicine; Society of Critical Care Medicine. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN) JPEN. 2009;33:277–316. doi: 10.1177/0148607109335234. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
