

Comparative effectiveness and cost-effectiveness of antiretroviral therapy and pre-exposure prophylaxis for HIV prevention in South Africa
- PMID: 24629217
- PMCID: PMC4003813
- DOI: 10.1186/1741-7015-12-46
Comparative effectiveness and cost-effectiveness of antiretroviral therapy and pre-exposure prophylaxis for HIV prevention in South Africa
Abstract
Background: Antiretroviral therapy (ART) and oral pre-exposure prophylaxis (PrEP) are effective in reducing HIV transmission in heterosexual adults. The epidemiologic impact and cost-effectiveness of combined prevention approaches in resource-limited settings remain unclear.
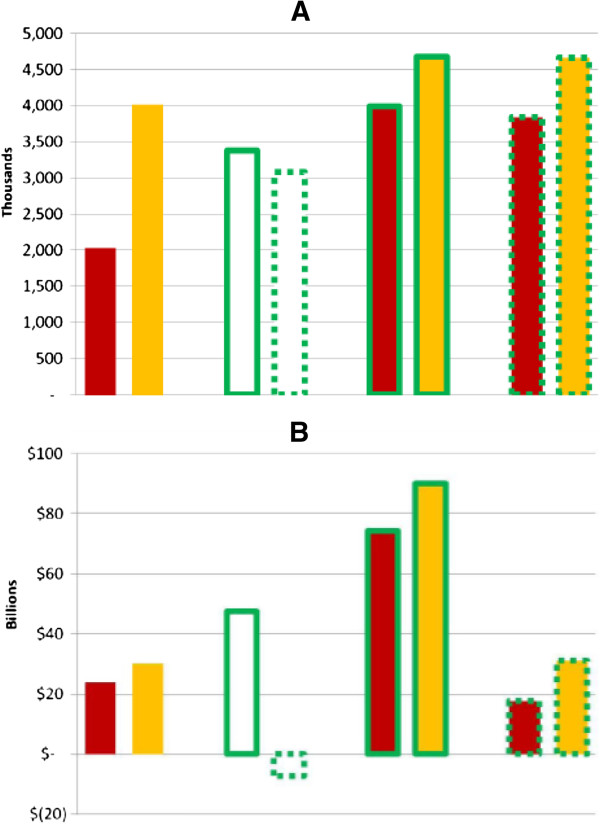
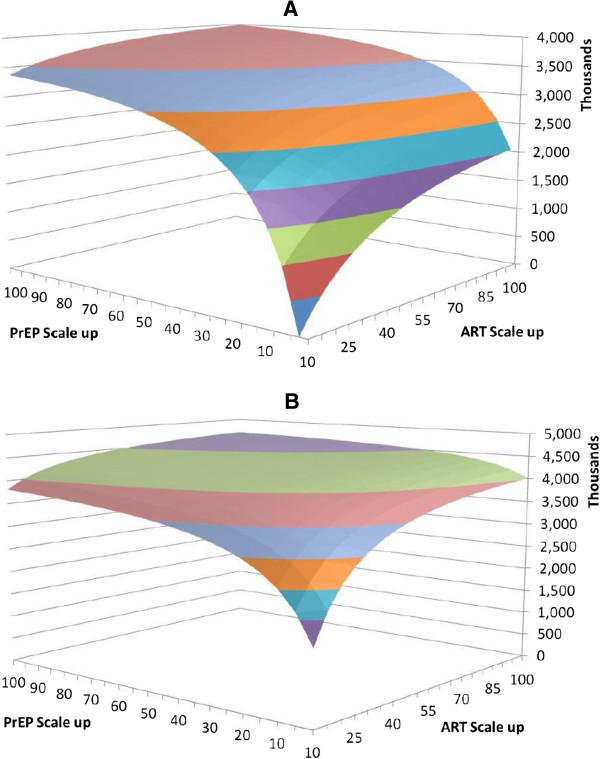
Methods: We develop a dynamic mathematical model of the HIV epidemic in South Africa's adult population. We assume ART reduces HIV transmission by 95% and PrEP by 60%. We model two ART strategies: scaling up access for those with CD4 counts ≤ 350 cells/μL (Guidelines) and for all identified HIV-infected individuals (Universal). PrEP strategies include use in the general population (General) and in high-risk individuals (Focused). We consider strategies where ART, PrEP, or both are scaled up to 100% of remaining eligible individuals yearly. We measure infections averted, quality-adjusted life-years (QALYs) gained and incremental cost-effectiveness ratios over 20 years.
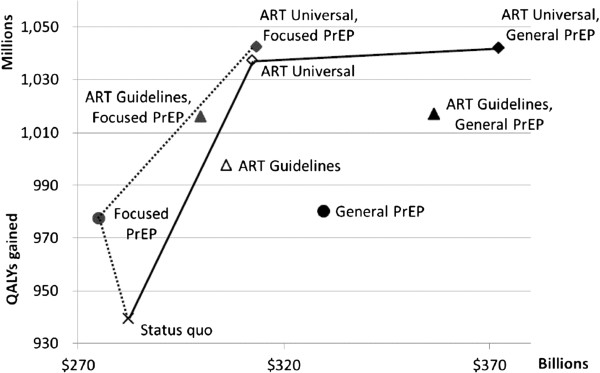
Results: Scaling up ART to 50% of eligible individuals averts 1,513,000 infections over 20 years (Guidelines) and 3,591,000 infections (Universal). Universal ART is the most cost-effective strategy at any scale ($160-$220/QALY versus comparable scale Guidelines ART expansion). General PrEP is costly and provides limited benefits beyond ART scale-up ($7,680/QALY to add 100% PrEP to 50% Universal ART). Cost-effectiveness of General PrEP becomes less favorable when ART is widely given ($12,640/QALY gained when added to 100% Universal ART). If feasible, Focused PrEP is cost saving or highly cost effective versus status quo and when added to ART strategies.
Conclusions: Expanded ART coverage to individuals in early disease stages may be more cost-effective than current guidelines. PrEP can be cost-saving if delivered to individuals at increased risk of infection.
Figures
References
-
- The Economist. AIDS: The 30 years war. The Economist. 2nd June 2011. [ http://www.economist.com/node/18772276]
-
- World Health Organization (WHO), Joint United Nations Programme on HIV/AIDS (UNAIDS), United Nations Children’s Fund (UNICEF) Progress Report 2011: Global HIV/AIDS Response: Epidemic Update and Health Sector Progress Towards Universal Access. Geneva, Switzerland: WHO; 2011.
-
- Institute for Health Metrics and Evaluation (IHME) Continued Growth as MDG Deadline Approaches. Seattle, WA: IHME; 2011. p. 2011.
-
- The Henry J. Kaiser Family Foundation. Budget Tracker: Status of U.S. Funding for Key Global Health Accounts. Menlo Park, CA: The Henry J. Kaiser Family Foundation; 2012.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
