

Default mode network mechanisms of transcranial magnetic stimulation in depression
- PMID: 24629537
- PMCID: PMC4209727
- DOI: 10.1016/j.biopsych.2014.01.023
Default mode network mechanisms of transcranial magnetic stimulation in depression
Abstract
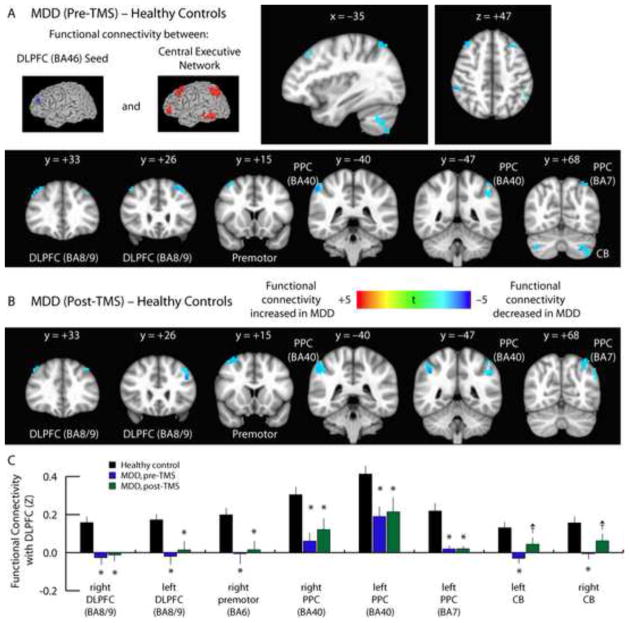
Background: Repetitive transcranial magnetic stimulation (TMS) of the dorsolateral prefrontal cortex (DLPFC) is an established treatment for depression, but its underlying mechanism of action remains unknown. Abnormalities in two large-scale neuronal networks-the frontoparietal central executive network (CEN) and the medial prefrontal-medial parietal default mode network (DMN)-are consistent findings in depression and potential therapeutic targets for TMS. Here, we assessed the impact of TMS on activity in these networks and their relation to treatment response.
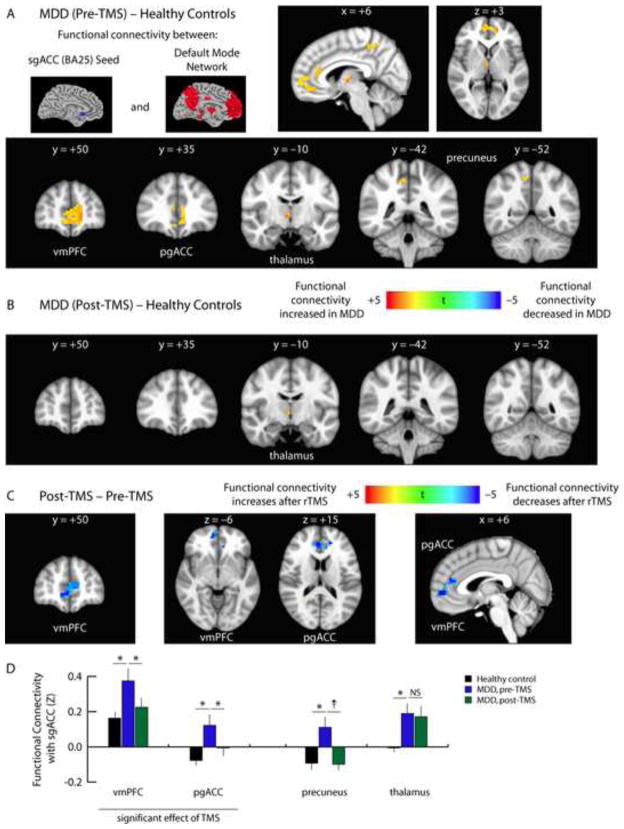
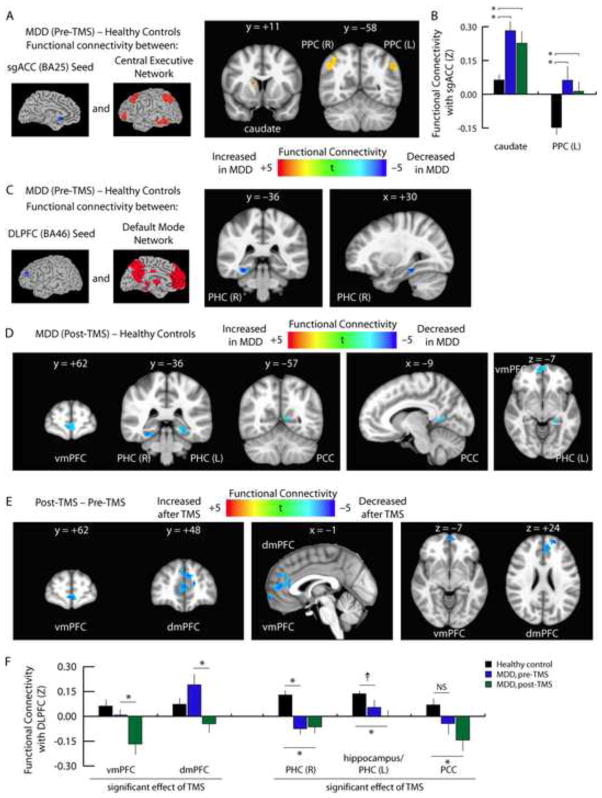
Methods: We used resting state functional magnetic resonance imaging to measure functional connectivity within and between the DMN and CEN in 17 depressed patients, before and after a 5-week course of TMS. Motivated by prior reports, we focused on connectivity seeded from the DLPFC and the subgenual cingulate, a key region closely aligned with the DMN in depression. Connectivity was also compared with a cohort of 35 healthy control subjects.
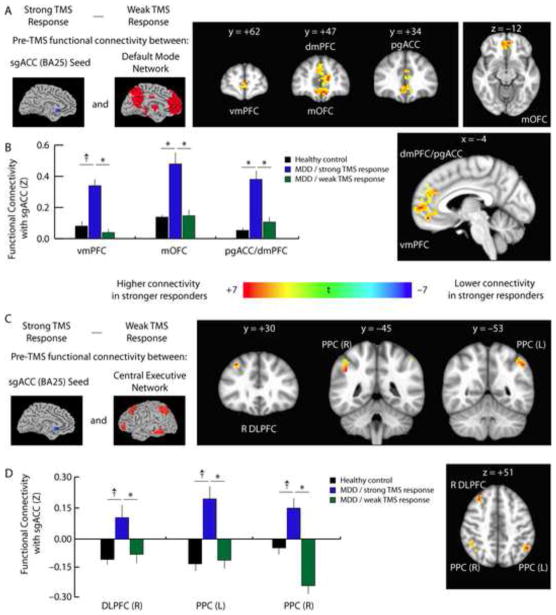
Results: Before treatment, functional connectivity in depressed patients was abnormally elevated within the DMN and diminished within the CEN, and connectivity between these two networks was altered. Transcranial magnetic stimulation normalized depression-related subgenual hyperconnectivity in the DMN but did not alter connectivity in the CEN. Transcranial magnetic stimulation also induced anticorrelated connectivity between the DLPFC and medial prefrontal DMN nodes. Baseline subgenual connectivity predicted subsequent clinical improvement.
Conclusions: Transcranial magnetic stimulation selectively modulates functional connectivity both within and between the CEN and DMN, and modulation of subgenual cingulate connectivity may play an important mechanistic role in alleviating depression. The results also highlight potential neuroimaging biomarkers for predicting treatment response.
Keywords: Central executive network; TMS; default mode network; depression; resting state fMRI.
Copyright © 2014 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- PascualLeone A, Rubio B, Pallardo F, Catala MD. Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet. 1996;348:233–237. - PubMed
-
- George MS, Lisanby SH, Avery D, McDonald WM, Durkalski V, Pavlicova M, et al. Daily Left Prefrontal Transcranial Magnetic Stimulation Therapy for Major Depressive Disorder A Sham-Controlled Randomized Trial. Archives of General Psychiatry. 2010;67:507–516. - PubMed
-
- Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. American Journal of Psychiatry. 2006;163:1905–1917. - PubMed
-
- Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: Implications for clinical practice. American Journal of Psychiatry. 2006;163:28–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
