

Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes
- PMID: 24629619
- PMCID: PMC4310561
- DOI: 10.1016/j.ophtha.2014.01.017
Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes
Abstract
Purpose: To compare the rates of retinal nerve fiber layer (RNFL) loss in patients suspected of having glaucoma who developed visual field damage (VFD) with those who did not develop VFD and to determine whether the rate of RNFL loss can be used to predict the development of VFD.
Design: Prospective, observational cohort study.
Participants: Glaucoma suspects, defined as having glaucomatous optic neuropathy or ocular hypertension (intraocular pressure, >21 mmHg) without repeatable VFD at baseline, from the Diagnostic Innovations in Glaucoma Study and the African Descent and Glaucoma Evaluation Study.
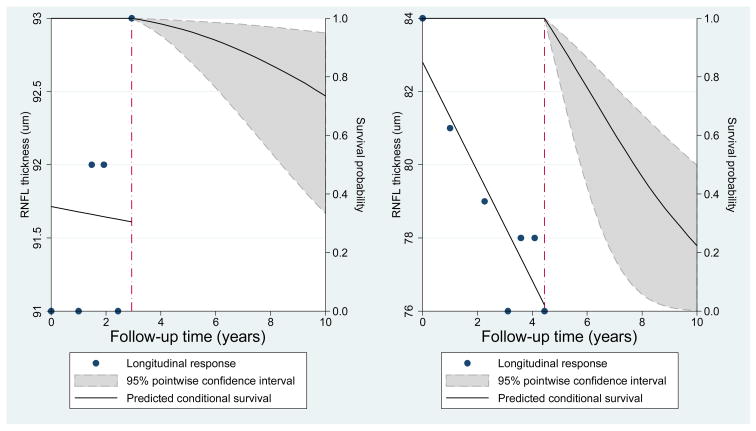
Methods: Global and quadrant RNFL thickness (RNFLT) were measured with the Spectralis spectral-domain optical coherence tomography (SD-OCT; Spectralis HRA+OCT [Heidelberg Engineering, Heidelberg, Germany]). Visual field damage was defined as having 3 consecutive abnormal visual fields. The rate of RNFL loss in eyes developing VFD was compared to eyes not developing VFD using multivariate linear mixed-effects models. A joint longitudinal survival model used the estimated RNFLT slope to predict the risk of developing VFD, while adjusting for potential confounding variables.
Main outcome measures: The rate of RNFL thinning and the probability of developing VFD.
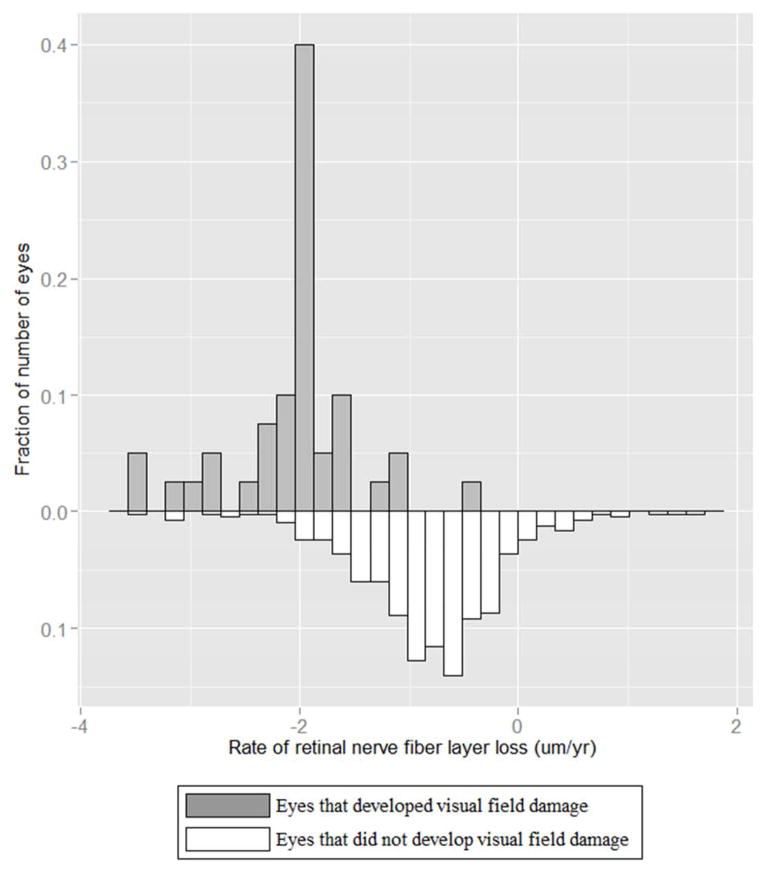
Results: Four hundred fifty-four eyes of 294 glaucoma suspects were included. The average number of SD-OCT examinations was 4.6 (range, 2-9), with median follow-up of 2.2 years (0.4-4.1 years). Forty eyes (8.8%) developed VFD. The estimated mean rate of global RNFL loss was significantly faster in eyes that developed VFD compared with eyes that did not develop VFD (-2.02 μm/year vs. -0.82 μm/year; P<0.001). The joint longitudinal survival model showed that each 1-μm/year faster rate of global RNFL loss corresponded to a 2.05-times higher risk of developing VFD (hazard ratio, 2.05; 95% confidence interval, 1.14-3.71; P = 0.017).
Conclusions: The rate of global RNFL loss was more than twice as fast in eyes that developed VFD compared with eyes that did not develop VFD. A joint longitudinal survival model showed that a 1-μm/year faster rate of RNFLT loss corresponded to a 2.05-times higher risk of developing VFD. These results suggest that measuring the rate of SD-OCT RNFL loss may be a useful tool to help identify patients who are at a high risk of developing visual field loss.
Copyright © 2014 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: No Disclosure (LS, PAS, NK, SJ, NH, HF)
Figures
References
-
- Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet. 2004;363:1711–20. - PubMed
-
- Kass M, Heuer D, Higginbotham E, et al. Ocular Hypertension Treatment Study Group. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–13. - PubMed
-
- European Glaucoma Prevention Study (EGPS) Group. Results of the European Glaucoma Prevention Study. Ophthalmology. 2005;112:366–75. - PubMed
-
- Flammer J, Drance S, Zulauf M. Differential light threshold: short- and long-term fluctuation in patients with glaucoma, normal controls, and patients with suspected glaucoma. Arch Ophthalmol. 1984;102:704–6. - PubMed
-
- Kutzko KE, Brito CF, Wall M. Effect of instructions on conventional automated perimetry. Invest Ophthalmol Vis Sci. 2000;41:2006–13. - PubMed
Publication types
MeSH terms
Grants and funding
- EY08208/EY/NEI NIH HHS/United States
- K23 EY013959/EY/NEI NIH HHS/United States
- P30 EY022589/EY/NEI NIH HHS/United States
- U10EY14267/EY/NEI NIH HHS/United States
- R01 EY019869/EY/NEI NIH HHS/United States
- P30EY022589/EY/NEI NIH HHS/United States
- EY13959/EY/NEI NIH HHS/United States
- EY022039/EY/NEI NIH HHS/United States
- R01 EY011008/EY/NEI NIH HHS/United States
- R01 EY021818/EY/NEI NIH HHS/United States
- R01 EY008208/EY/NEI NIH HHS/United States
- EY021818/EY/NEI NIH HHS/United States
- EY019869/EY/NEI NIH HHS/United States
- EY11008/EY/NEI NIH HHS/United States
- U10 EY014267/EY/NEI NIH HHS/United States
- R01 EY022039/EY/NEI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
