

Additional value of transluminal attenuation gradient in CT angiography to predict hemodynamic significance of coronary artery stenosis
- PMID: 24631509
- PMCID: PMC4378651
- DOI: 10.1016/j.jcmg.2013.12.013
Additional value of transluminal attenuation gradient in CT angiography to predict hemodynamic significance of coronary artery stenosis
Abstract
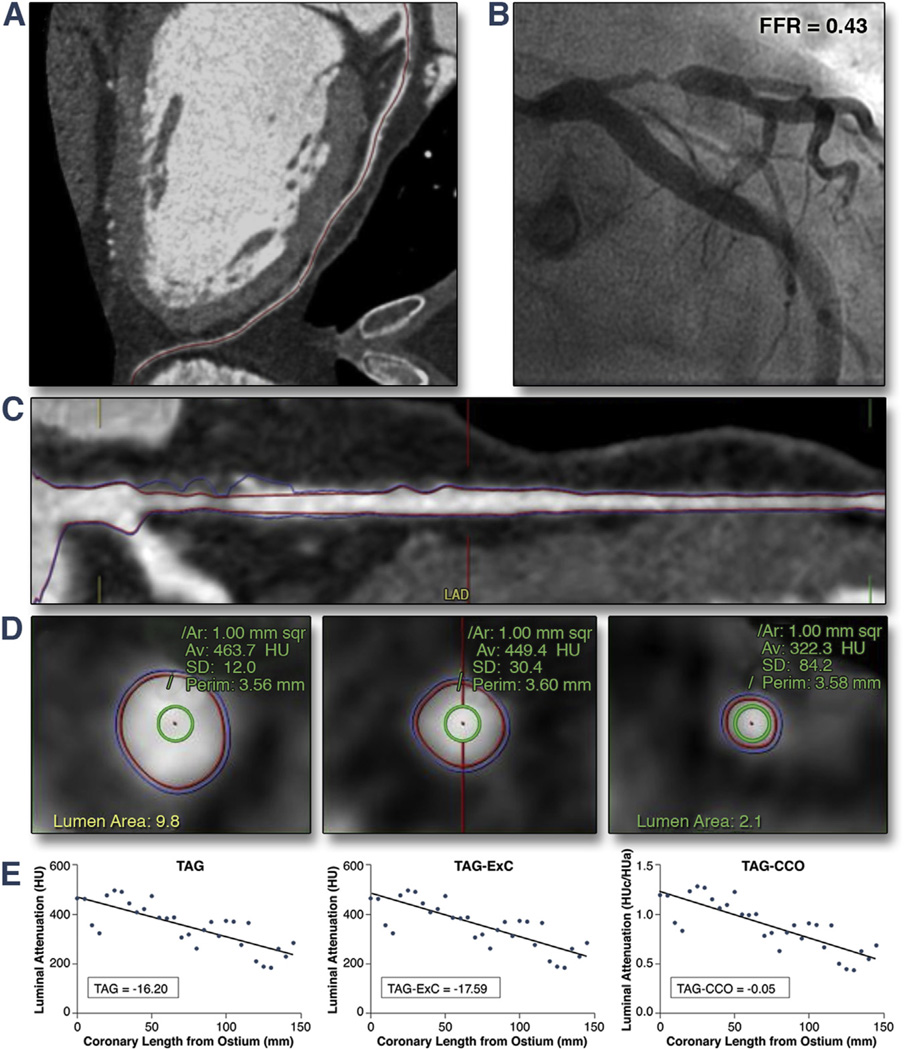
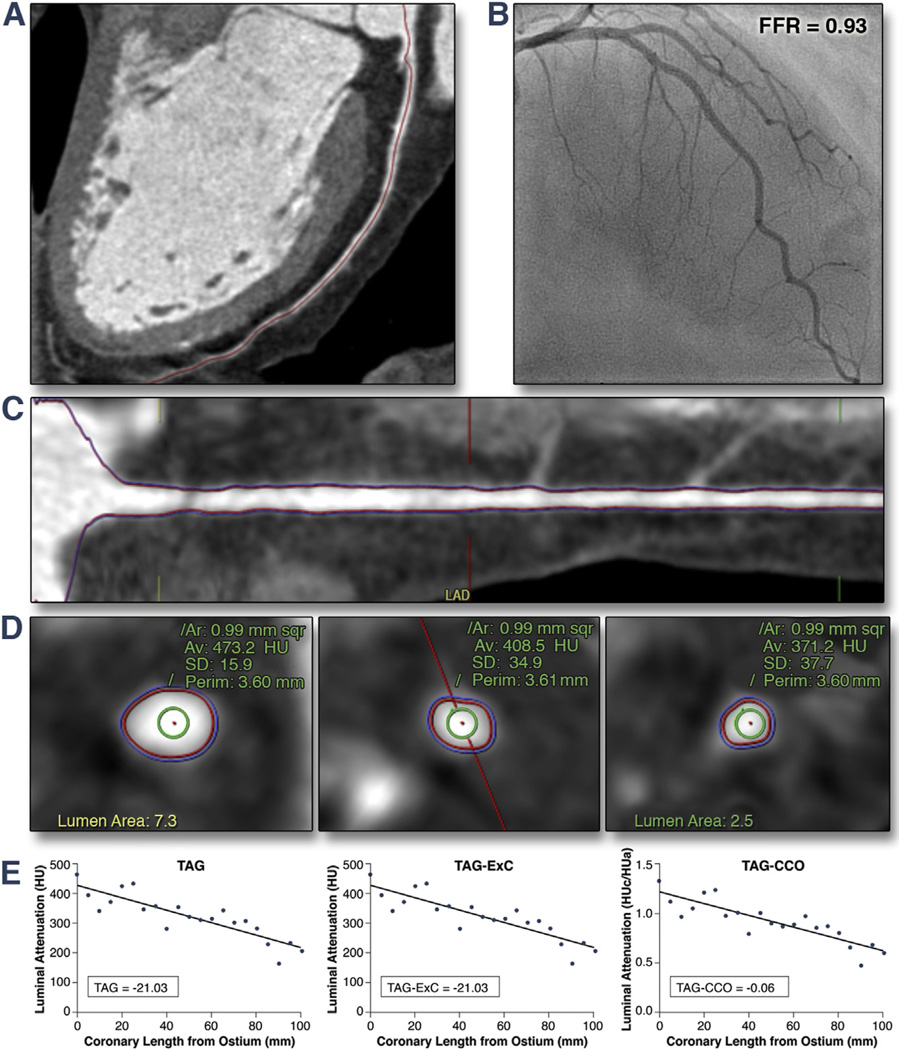
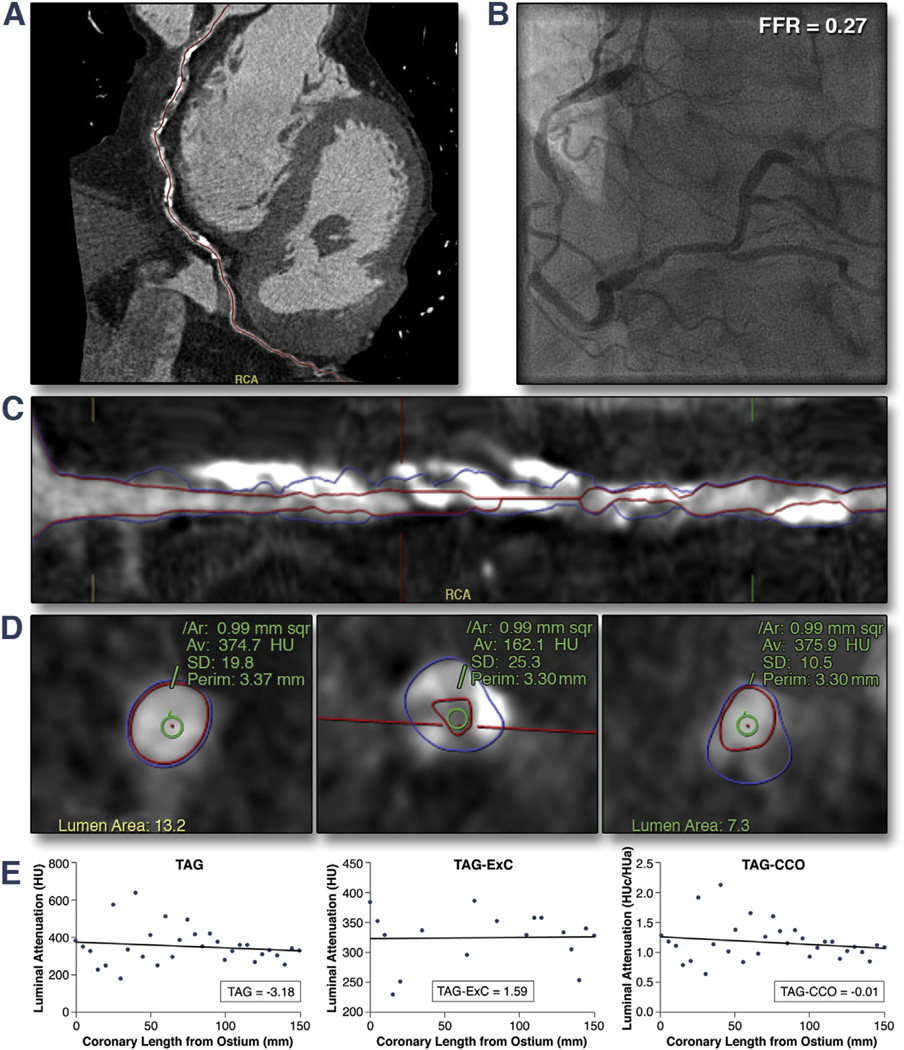
Objectives: The current study evaluates the incremental value of transluminal attenuation gradient (TAG), TAG with corrected contrast opacification (CCO), and TAG with exclusion of calcified coronary segments (ExC) over coronary computed tomography angiogram (CTA) alone using fractional flow reserve (FFR) as the gold standard.
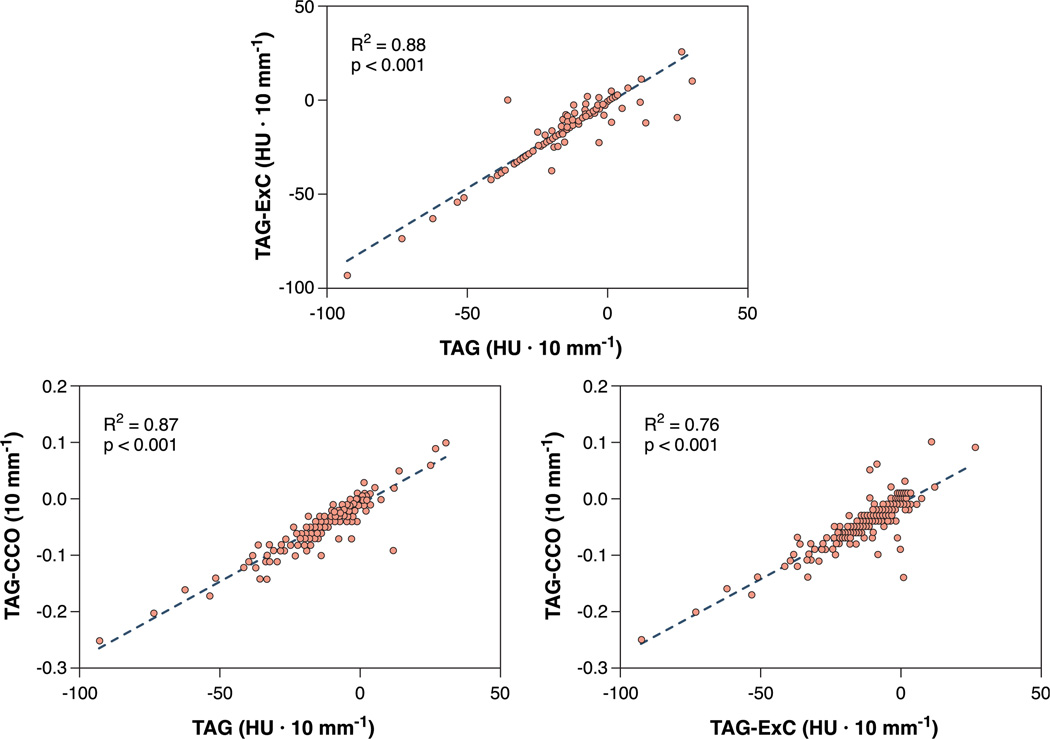
Background: TAG is defined as the contrast opacification gradient along the length of a coronary artery on a coronary CTA. Preliminary data suggest that TAG provides additional functional information. Interpretation of TAG is hampered by multiple heartbeat acquisition algorithms and coronary calcifications. Two correction models have been proposed based on either dephasing of contrast delivery by relating coronary density to corresponding descending aortic opacification (TAG-CCO) or excluding calcified coronary segments (TAG-ExC).
Methods: Eighty-five patients with intermediate probability of coronary artery disease were prospectively included. All patients underwent step-and-shoot 256-slice coronary CTA. TAG, TAG-CCO, and TAG-ExC analyses were performed followed by invasive coronary angiography in conjunction with FFR measurements of all major coronary branches.
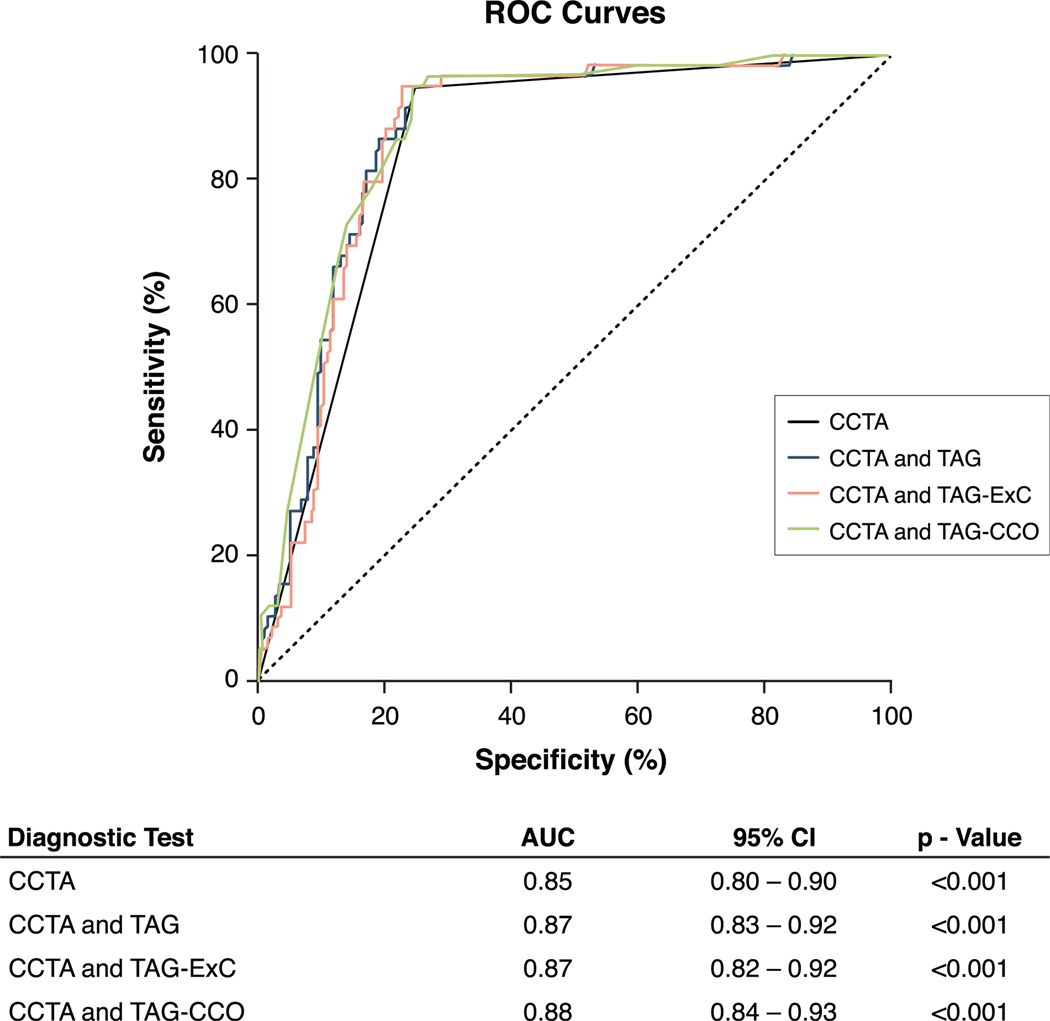
Results: Thirty-four patients (40%) were diagnosed with hemodynamically-significant coronary artery disease (i.e., FFR ≤0.80). On a per-vessel basis (n = 253), 59 lesions (23%) were graded as hemodynamically significant, and the diagnostic accuracy of coronary CTA (diameter stenosis ≥50%) was 95%, 75%, 98%, and 54% for sensitivity, specificity, negative predictive value, and positive predictive value, respectively. TAG and TAG-ExC did not discriminate between vessels with or without hemodynamically significant lesions (-13.5 ± 17.1 HU [Hounsfield units] × 10 mm(-1) vs. -11.6 ± 13.3 HU × 10 mm(-1), p = 0.36; and 13.1 ± 15.9 HU × 10 mm(-1) vs. -11.4 ± 11.7 HU × 10 mm(-1), p = 0.77, respectively). TAG-CCO was lower in vessels with a hemodynamically-significant lesion (-0.050 ± 0.051 10 mm(-1) vs. -0.036 ± 0.034 10 mm(-1), p = 0.03) and TAG-ExC resulted in a slight improvement of the net reclassification index (0.021, p < 0.05).
Conclusions: TAG did not provide incremental diagnostic value over 256-slice coronary CTA alone in assessing the hemodynamic consequences of a coronary stenosis. Correction for temporal nonuniformity of contrast delivery or exclusion of calcified coronary segments slightly enhanced the results.
Keywords: coronary artery disease; coronary computed tomography angiography; fractional flow reserve.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Arbab-Zadeh A, Miller JM, Rochitte CE, et al. Diagnostic accuracy of computed tomography coronary angiography according to pre-test probability of coronary artery disease and severity of coronary arterial calcification: the CORE-64 (Coronary Artery Evaluation Using 64-Row Multidetector Computed Tomography Angiography) International Multicenter Study. J Am Coll Cardiol. 2012;59:379–387. - PMC - PubMed
-
- Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008;52:1724–1732. - PubMed
-
- Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52:2135–2144. - PubMed
-
- Danad I, Raijmakers PG, Harms HJ, et al. Effect of cardiac hybrid 15O-water PET/CT imaging on downstream referral for invasive coronary angiography and revascularization rate. Eur Heart J Cardiovasc Imaging. 2014;15:170–179. - PubMed
-
- Schuijf JD, Wijns W, Jukema JW, et al. Relationship between noninvasive coronary angiography with multi-slice computed tomography and myocardial perfusion imaging. J Am Coll Cardiol. 2006;48:2508–2514. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
