

Ablation of rotor and focal sources reduces late recurrence of atrial fibrillation compared with trigger ablation alone: extended follow-up of the CONFIRM trial (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation)
- PMID: 24632280
- PMCID: PMC4008643
- DOI: 10.1016/j.jacc.2014.02.543
Ablation of rotor and focal sources reduces late recurrence of atrial fibrillation compared with trigger ablation alone: extended follow-up of the CONFIRM trial (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation)
Abstract
Objectives: The aim of this study was to determine if ablation that targets patient-specific atrial fibrillation (AF)-sustaining substrates (rotors or focal sources) is more durable than trigger ablation alone at preventing late AF recurrence.
Background: Late recurrence substantially limits the efficacy of pulmonary vein isolation for AF and is associated with pulmonary vein reconnection and the emergence of new triggers.
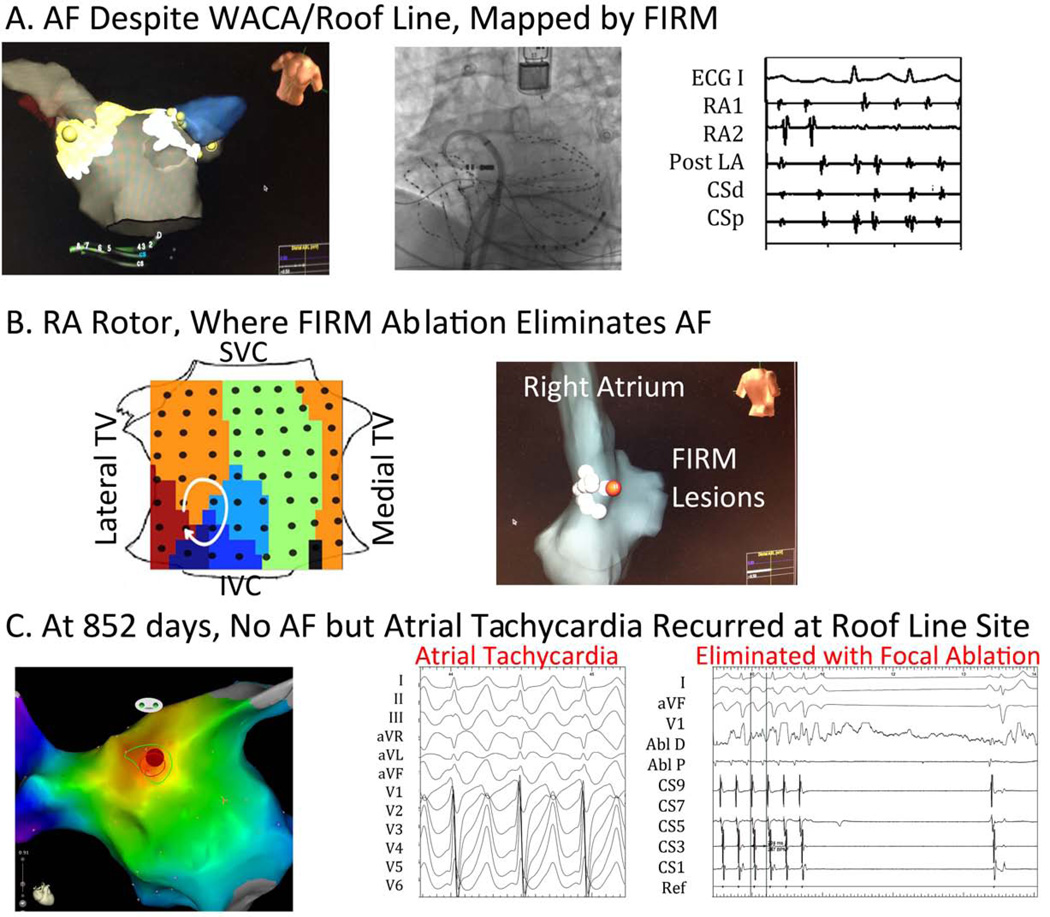
Methods: Three-year follow-up was performed of the CONFIRM (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) trial, in which 92 consecutive patients with AF (70.7% persistent) underwent novel computational mapping. Ablation comprised source (focal impulse and rotor modulation [FIRM]) and then conventional ablation in 27 patients (FIRM guided) and conventional ablation alone in 65 patients (FIRM blinded). Patients were followed with implanted electrocardiographic monitors when possible (85.2% of FIRM-guided patients, 23.1% of FIRM-blinded patients).
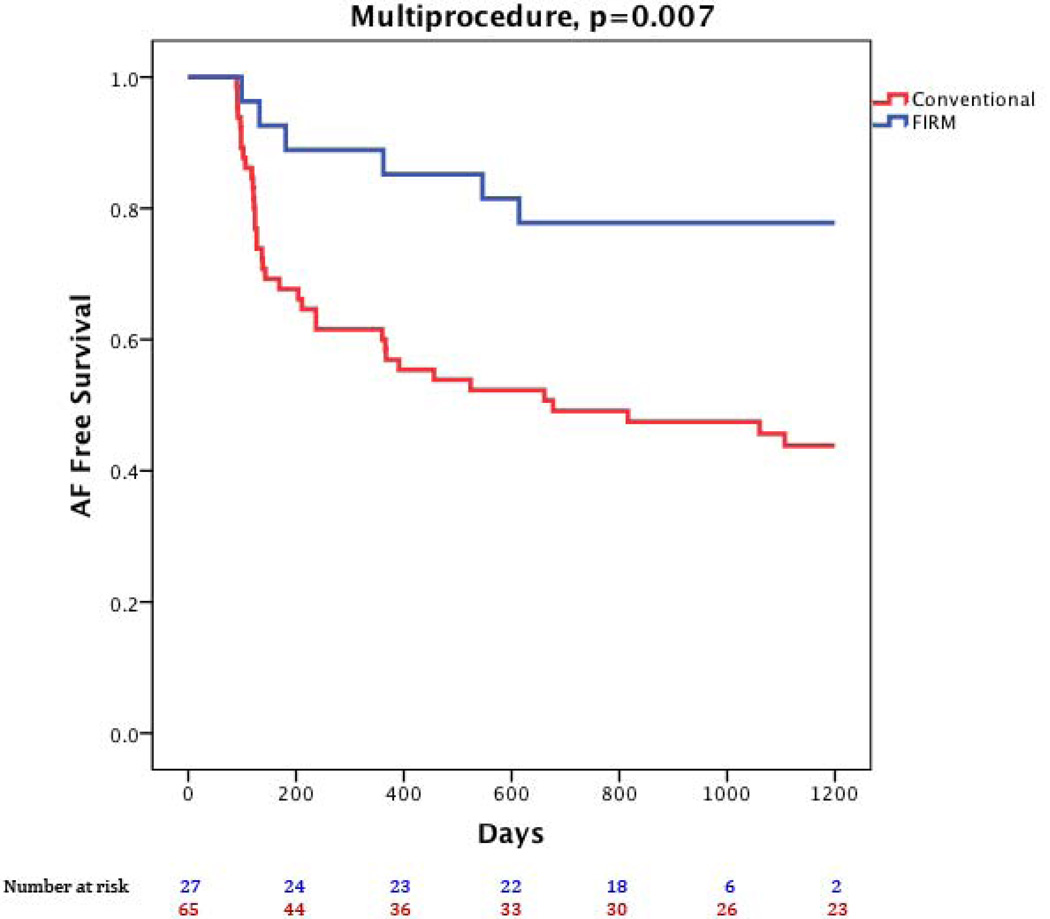
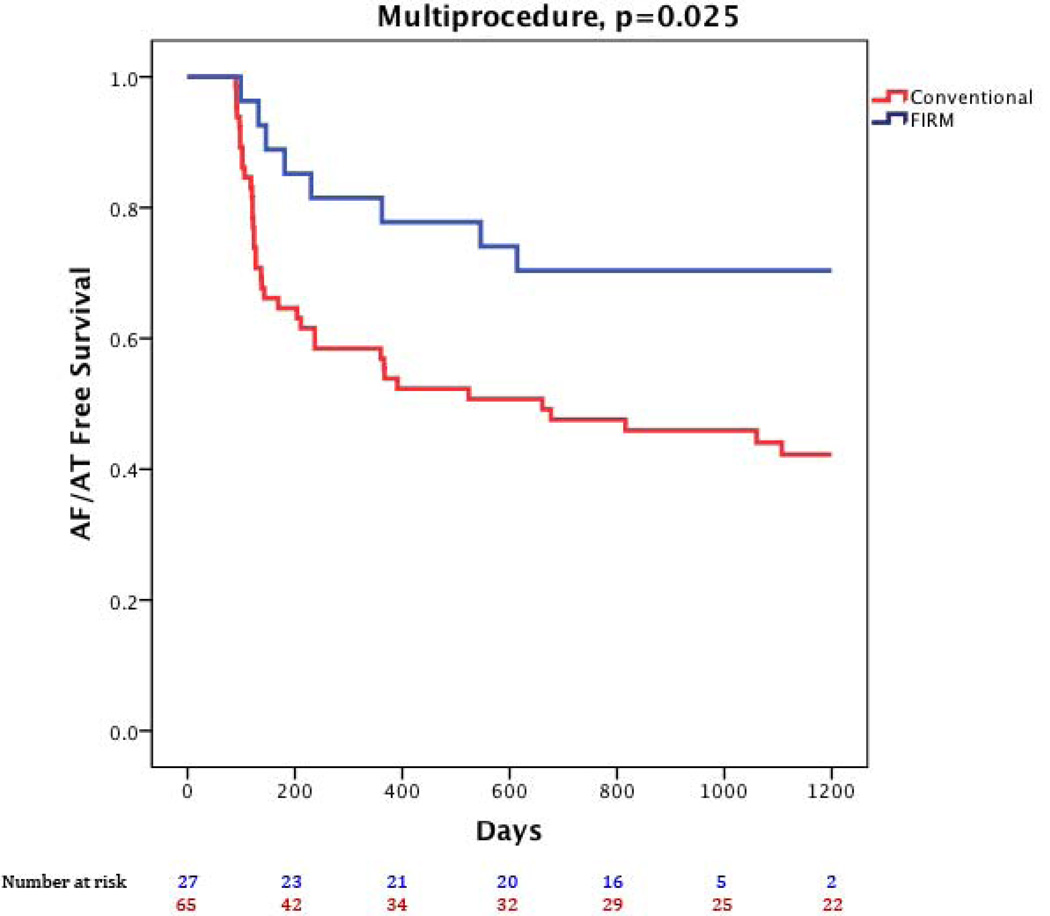
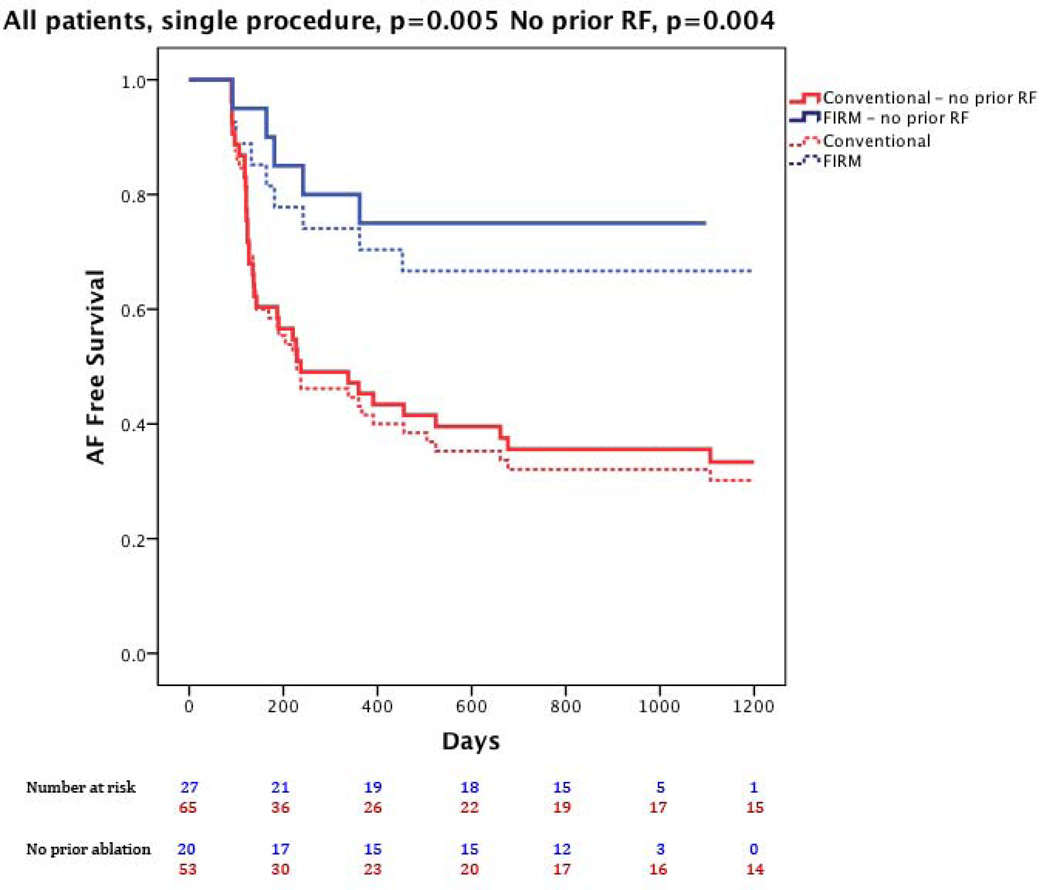
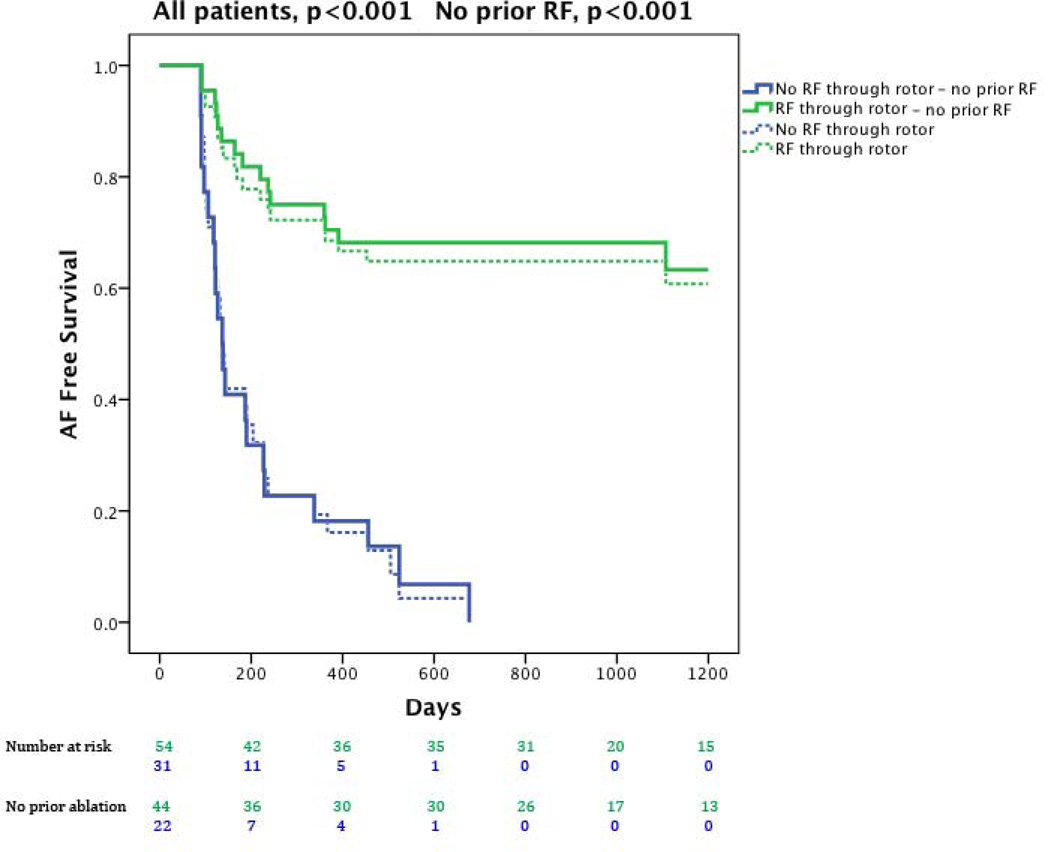
Results: FIRM mapping revealed a median of 2 (interquartile range: 1 to 2) rotors or focal sources in 97.7% of patients during AF. During a median follow-up period of 890 days (interquartile range: 224 to 1,563 days), compared to FIRM-blinded therapy, patients receiving FIRM-guided ablation maintained higher freedom from AF after 1.2 ± 0.4 procedures (median 1; interquartile range: 1 to 1) (77.8% vs. 38.5%, p = 0.001) and a single procedure (p < 0.001) and higher freedom from all atrial arrhythmias (p = 0.003). Freedom from AF was higher when ablation directly or coincidentally passed through sources than when it missed sources (p < 0.001).
Conclusions: FIRM-guided ablation is more durable than conventional trigger-based ablation in preventing 3-year AF recurrence. Future studies should investigate how ablation of patient-specific AF-sustaining rotors and focal sources alters the natural history of arrhythmia recurrence. (The Dynamics of Human Atrial Fibrillation; NCT01008722).
Keywords: FIRM; ablation; atrial fibrillation; clinical trial; electrical rotors.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Calkins CH. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Patient Selection, Procedural Techniques, Patient Management and Follow-up, Definitions, Endpoints, and Research Trial Design. Heart Rhythm. 2012;9:632–696.
-
- Roy D, Talajic M, Nattel S, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667–2677. - PubMed
-
- Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362:1363–1373. - PubMed
-
- Weerasooriya R, Khairy P, Litalien J, et al. Catheter ablation for atrial fibrillation: Are results maintained at 5 years of follow-up? J Am Coll Cardiol. 2011;57:160–166. - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333–340. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
