

Hospital variation in noninvasive positive pressure ventilation for acute decompensated heart failure
- PMID: 24633829
- PMCID: PMC4386575
- DOI: 10.1161/CIRCHEARTFAILURE.113.000698
Hospital variation in noninvasive positive pressure ventilation for acute decompensated heart failure
Abstract
Background: Although noninvasive positive pressure ventilation (NIPPV) for patients with acute decompensated heart failure was introduced almost 20 years ago, the variation in its use among hospitals remains unknown. We sought to define hospital practice patterns of NIPPV use for acute decompensated heart failure and their relationship with intubation and mortality.
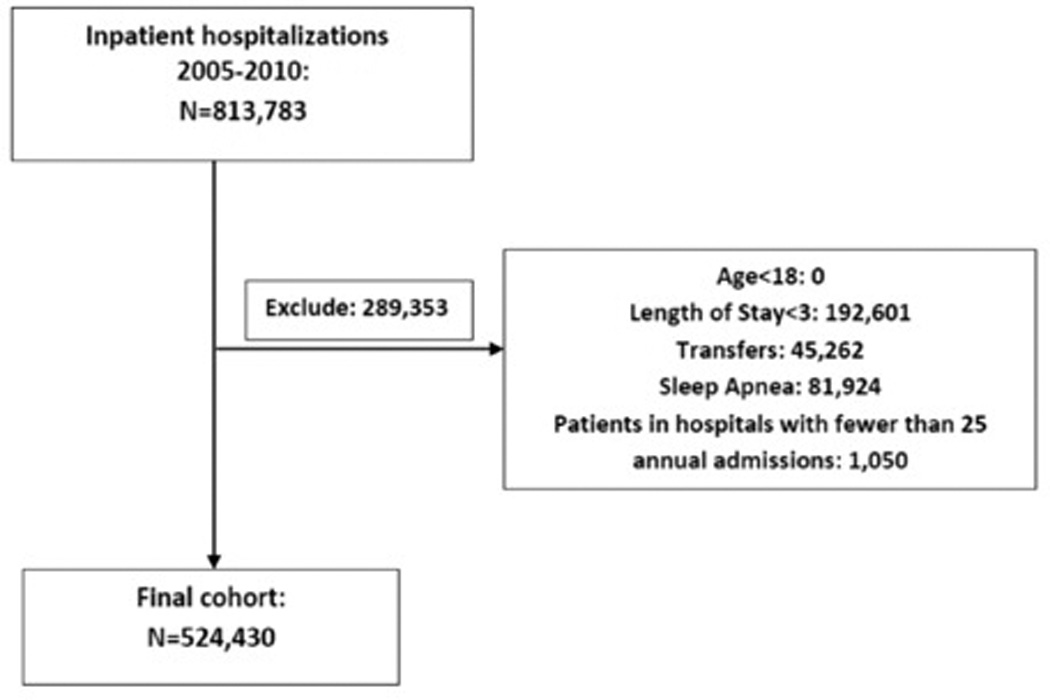
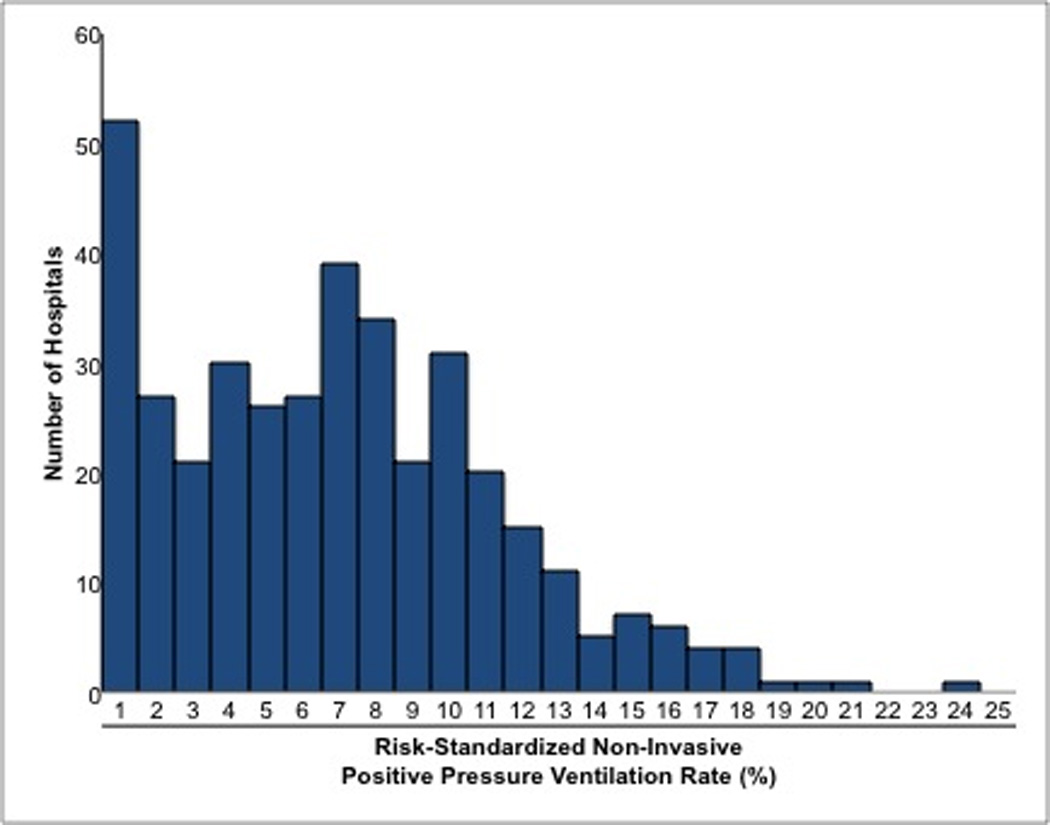
Methods and results: We conducted a cross-sectional study using a database maintained by Premier, Inc., that includes a date-stamped log of all billed items for hospitalizations at >400 hospitals. We examined hospitalizations for acute decompensated heart failure in this database from 2005 to 2010 and included hospitals with annual average volume of >25 such hospitalizations. We identified 384 hospitals that encompassed 524 430 hospitalizations (median annual average volume: 206). We used hierarchical logistic regression models to calculate hospital-level outcomes: risk-standardized NIPPV rate, risk-standardized intubation rate, and in-hospital risk-standardized mortality rate. We grouped hospitals into quartiles by risk-standardized NIPPV rate and compared risk-standardized mortality rates and risk-standardized intubation rates across quartiles. Median risk-standardized NIPPV rate was 6.2% (interquartile range, 2.8%-9.3%; 5th percentile, 0.2%; 95th percentile, 14.8%). There was no clear pattern of risk-standardized mortality rates across quartiles. The bottom quartile of hospitals had higher risk-standardized intubation rate (11.4%) than each of the other quartiles (9.0%, 9.7%, and 9.1%; P<0.02 for all comparisons).
Conclusions: Substantial variation exists among hospitals in the use of NIPPV for acute decompensated heart failure without evidence for differences in mortality. There may be a threshold effect in relation to intubation rates, with the lowest users of NIPPV having higher intubation rates.
Keywords: heart failure; mortality; ventilation.
© 2014 American Heart Association, Inc.
Conflict of interest statement
The other authors report no conflicts.
Figures
References
-
- Gray A, Goodacre S, Newby DE, Masson M, Sampson F, Nicholl J. Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2008;359:142–151. - PubMed
-
- Peter JV, Moran JL, Phillips-Hughes J, Graham P, Bersten AD. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006;367:1155–1163. - PubMed
-
- Weng C, Zhao YT, Liu QH, Fu CJ, Sun F, Ma YL, Chen YW, He QY. Meta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med. 2010;152:590–600. - PubMed
-
- Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation. 2009;119:1977–2016. - PubMed
-
- Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Katz SD, Klapholz M, Moser DK, Rogers JG, Starling RC, Stevenson WG, Tang WH, Teerlink JR, Walsh MN. Executive summary: HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. 2010;16:e1–e194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
